

Toxic Shock Syndrome Triggered by Thoracic Drain Insertion: A Pediatric Case Report
- PMID: 40661331
- PMCID: PMC12256205
- DOI: 10.70352/scrj.cr.25-0226
Toxic Shock Syndrome Triggered by Thoracic Drain Insertion: A Pediatric Case Report
Abstract
Introduction: Postoperative Staphylococcus and streptococcal toxic shock syndrome (TSS) are associated with significant morbidity and mortality rates. As a result, surgical awareness is required to recognize and treat TSS appropriately. We report a pediatric case of TSS after thoracentesis for a pneumothorax.
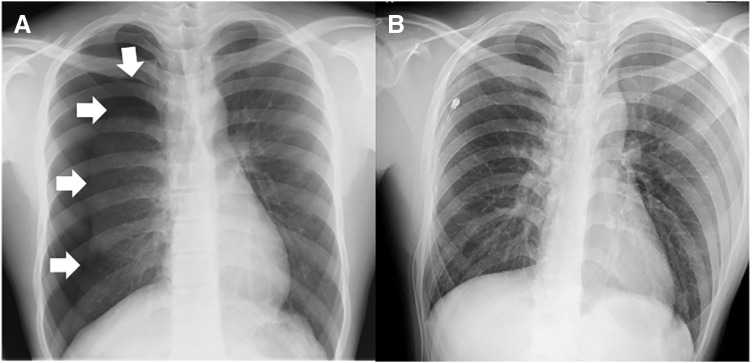
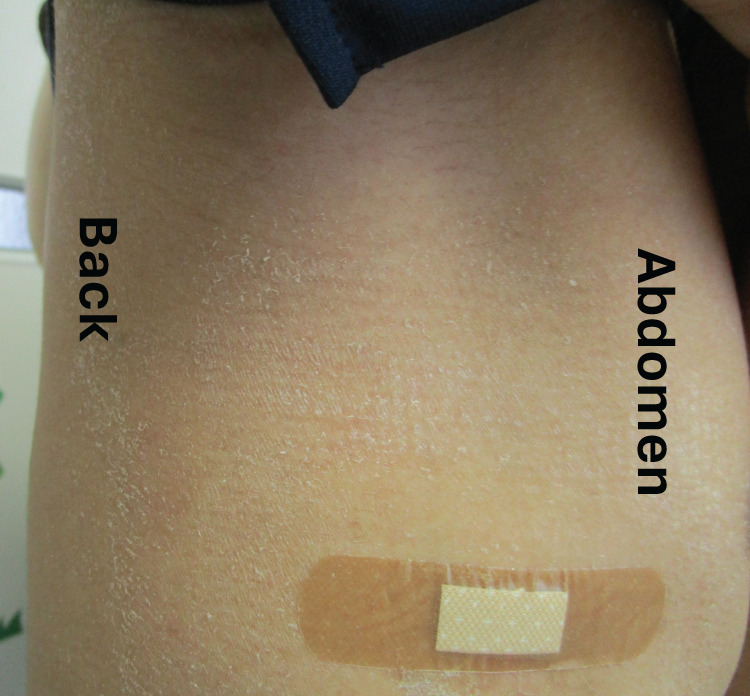
Case presentation: A 14-year-old boy was diagnosed with a right pneumothorax and underwent thoracentesis with a trocar catheter. After 2 days, the patient developed a fever, headache, vomiting, and diarrhea. No obvious contamination of the drain puncture wound was observed. He was diagnosed with acute gastroenteritis and received intravenous treatment. On the 4th day after drainage, his blood pressure decreased. Due to suspected septic shock, he was transferred to the intensive care unit and administered antibiotics, immunoglobulin, and a hypertensive agent. His treatment response was good, and his general condition improved relatively quickly. On the 6th day, the patient was discharged from the intensive care unit. Although the air leak from the thoracic drain disappeared on day 3, the drain remained in place until day 8. Blood cultures obtained at the time of septic shock were all negative; however, pleural fluid and thoracic drain tip cultures detected Staphylococcus aureus, and the production of TSS toxin-1 and enterotoxin type C was confirmed. Retrospectively, the patient was diagnosed with TSS triggered by the insertion of a thoracic drain. He was discharged from the hospital on day 11. After discharge, he experienced skin desquamation of the axilla and buttocks. The patient also reported diffuse erythematous eczema on day 3 after drainage. He received antimicrobial therapy for 14 days and recovered fully without any complications.
Conclusions: TSS can occur after simple, routine procedures such as thoracentesis. Symptoms such as fever, rash, vomiting, and diarrhea should raise concern for TSS and prompt further exploration and cultures, even in benign-appearing postoperative wounds.
Keywords: chest drain; pneumothorax; toxic shock syndrome.
© 2025 The Author(s). Published by Japan Surgical Society.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- CDC. Toxic Shock Syndrome (Other Than Streptococcal) (TSS) 2011 Case Definition.
-
- Broome CV. Epidemiology of toxic shock syndrome in the United States: overview. Clin Infect Dis 1989; 11: S14–21. - PubMed
-
- Descloux E, Perpoint T, Ferry T, et al. One in five mortality in non-menstrual toxic shock syndrome versus no mortality in menstrual cases in a balanced French series of 55 cases. Eur J Clin Microbiol Infect Dis 2008; 27: 37–43. - PubMed
-
- Graham DR, O’Brien M, Hayes JM, et al. Postoperative toxic shock syndrome. Clin Infect Dis 1995; 20: 895–9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials