Sensory neuron-expressed FGF13 controls nociceptive signaling in diabetic neuropathy models
- PMID: 40662354
- PMCID: PMC12259270
- DOI: 10.1172/JCI183749
Sensory neuron-expressed FGF13 controls nociceptive signaling in diabetic neuropathy models
Abstract
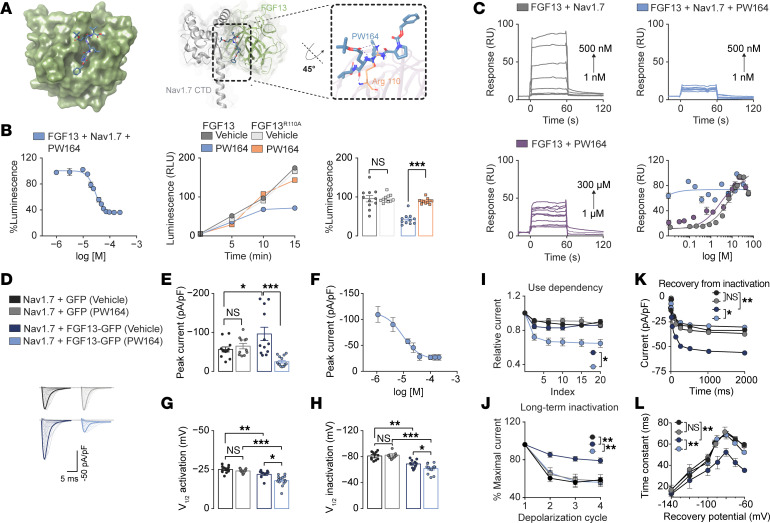
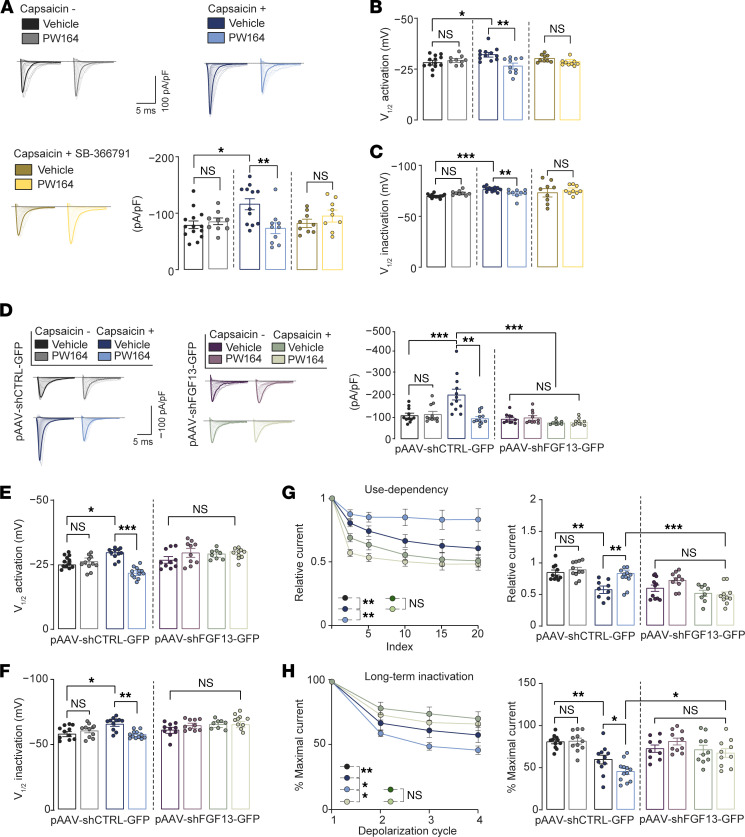
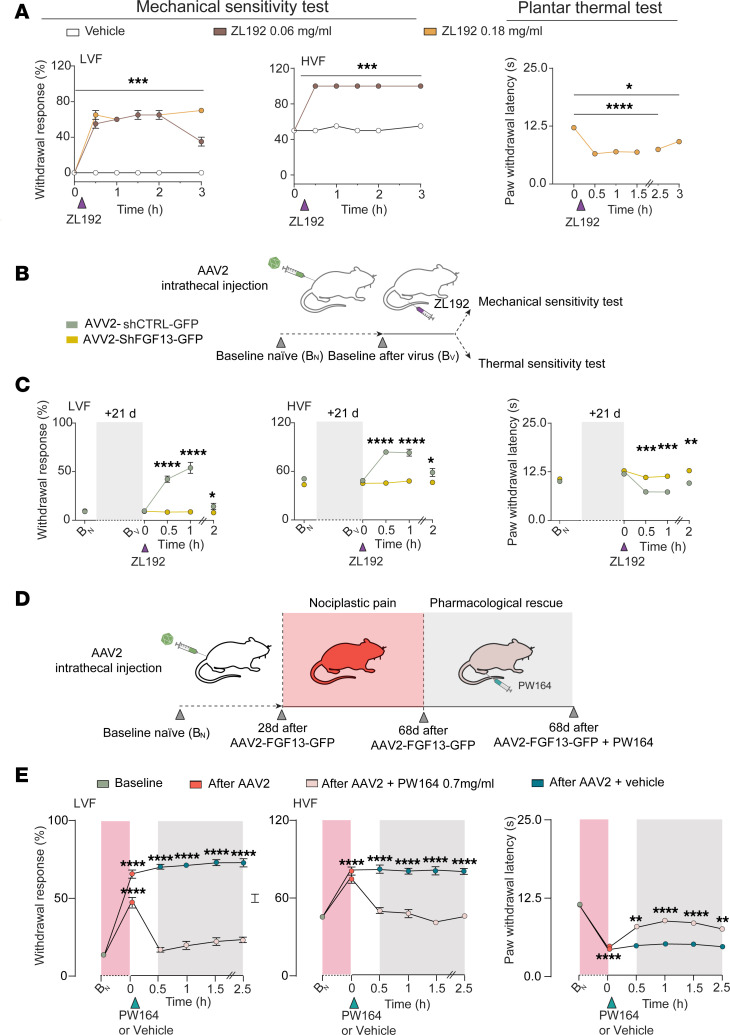
Nociception involves complex signaling, yet intrinsic mechanisms bidirectionally regulating this process remain unexplored. Here, we show that the fibroblast growth factor 13 (FGF13)/Nav1.7 protein-protein interaction (PPI) complex bidirectionally modulates nociception, and that the FGF13/Nav1.7 ratio is upregulated in type 2 diabetic neuropathy (T2DN). PW164, an FGF13/Nav1.7 channel C-terminal tail domain (CTD) PPI interface inhibitor, which reduces complex assembly, selectively suppressed Na+ currents sensitized by capsaicin-induced activation of TRPV1 channels in human induced pluripotent stem cell-derived (hIPSC-derived) sensory neurons and inhibited mechanical and thermal hyperalgesia in mice. FGF13 silencing mimics PW164 activity in culture and in vivo. Conversely, ZL192, an FGF13 ligand that stabilizes FGF13/Nav1.7 CTD assembly, sensitized Na+ currents in hIPSC-derived sensory neurons and exerted pronociceptive behavioral responses in mice. ZL192's effects were abrogated by FGF13 silencing in culture and in vivo and recapitulated by FGF13 overexpression. In a model of T2DN, PW164 injection reduced mechanical hyperalgesia locally and contralaterally without systemic side effects. In donor-derived dorsal root ganglia neurons, FGF13 and Nav1.7 proteins colocalized, and the FGF13/Nav1.7 protein ratio was upregulated in patients with T2DN. Lastly, we found that SCN9A variant V1831F, associated with painless diabetic neuropathy, abolished PW164-directed modulation of the FGF13/Nav1.7 PPI interface. Thus, FGF13 is a rheostat of nociception and promising therapeutic target for diabetic neuropathy pain.
Keywords: Neuroscience; Pain; Public Health; Sodium channels.
Figures