

Association between preoperative proton pump inhibitor use and postoperative infectious and renal complications following major elective surgery
- PMID: 40664466
- PMCID: PMC12279390
- DOI: 10.1503/cjs.010224
Association between preoperative proton pump inhibitor use and postoperative infectious and renal complications following major elective surgery
Abstract
Background: Use of poton pump inhibitors (PPIs) is associated with increased risk of Clostridioides difficile-associated colitis, pneumonia, and acute kidney injury. Their effect on postoperative complications is unknown. The objective of this study was to investigate the association between PPIs and the risk of C. difficile-associated colitis, pneumonia, and acute kidney injury following elective surgery.
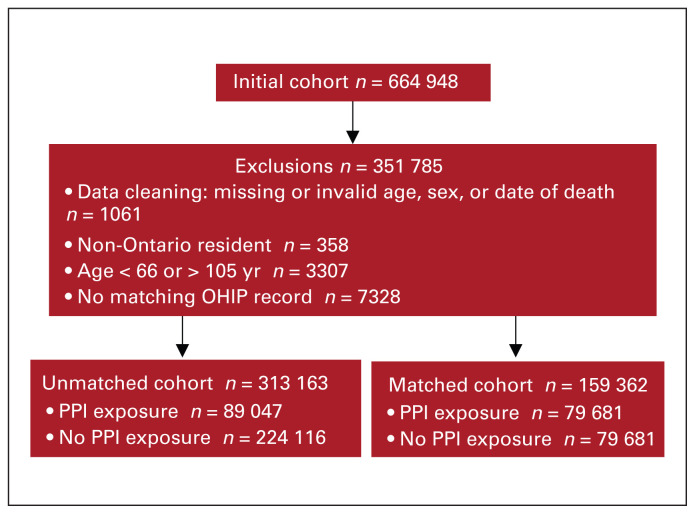
Methods: In this population-based, matched cohort study, we identified patients who had filled a PPI prescription within 90 days before major elective surgery (2010-2019). Study outcomes included C. difficile-associated colitis, pneumonia, acute kidney injury, gastrointestinal bleeding, and death within 90 days of surgery. We matched patients 1-to-1 on the basis of age, sex, procedure, date of surgery, and a propensity score predicting PPI exposure. We used logistic regression to evaluate between-group differences.
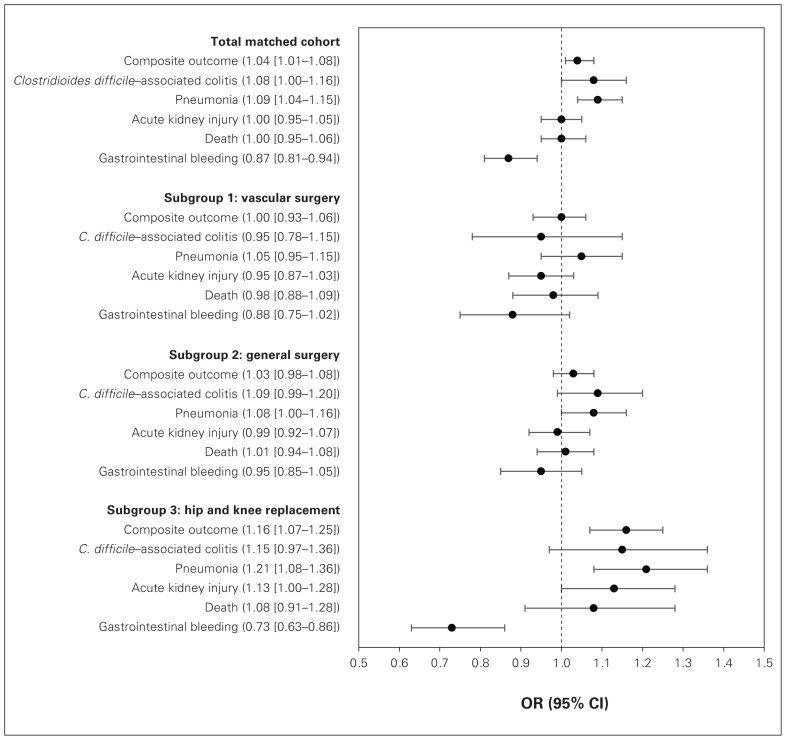
Results: Of 313 163 patients, 89 047 (28.4%) used PPIs; of those, 79 681 were successfully matched to patients who did not use PPIs. The risk of the composite outcome (acute kidney injury, pneumonia, C. difficile-associated colitis, and death) among the patients who used PPIs was slightly higher than among the patients who did not use PPIs (10.6% v. 10.2 4%), and was driven primarily by a higher rate of pneumonia among those who used PPIs (4.0% v. 3.7%). There was a lower rate of gastrointestinal bleeding among the patients who used PPIs (1.6% v. 1.8%). The risk of pneumonia was most pronounced in the subgroup undergoing hip and knee replacement (odds ratio 1.21, 95% confidence interval 1.08-1.36; p = 0.001). There were no significant differences between groups with regard to rates of C. difficile-associated colitis or acute kidney injury.
Conclusion: We found that preoperative PPI use was associated with higher rates of pneumonia, particularly among patients undergoing hip and knee replacement surgery, and lower rates of gastrointestinal bleeding. Patients taking a PPI before surgery should be targeted for therapies aimed at reducing pneumonia risk, such as aggressive chest physiotherapy, following their operation.
Contexte:: Les inhibiteurs de la pompe à protons (IPP) sont associés à un risque accru de colite à Clostridioides difficile, de pneumonie et d’insuffisance rénale aiguë. Leur effet sur les complications postopératoires est inconnu. Cette étude avait pour objectif d’explorer le lien entre les IPP et le risque de colite à C. difficile, de pneumonie et d’insuffisance rénale aiguë après une chirurgie non urgente.
Méthodes:: Dans cette étude de cohorte appariée basée dans la population, nous avons recensé la patientèle ayant fait exécuter une ordonnance d’IPP dans les 90 jours précédant une chirurgie majeure non urgente (2010–2019). Les paramètres de l’étude incluaient la colite à C. difficile, la pneumonie, l’insuffisance rénale aiguë, les saignements gastro-intestinaux et la mortalité dans les 90 jours suivant la chirurgie. Nous avons procédé à un appariement 1:1 des malades selon l’âge, le sexe, l’intervention, la date de la chirurgie et le score de propension indiquant une exposition aux IPP. Nous avons utilisé l’analyse de régression logistique pour évaluer les différences entre les groupes.
Résultats:: Parmi les 313 163 patientes et patients, 89 047 (28,4 %) utilisaient des IPP; parmi eux, 79 681 ont pu être appariés à des patientes et patients n’en faisant pas usage. Le risque d’occurrence d’un paramètre mixte (insuffisance rénale aiguë, pneumonie, colite à C. difficile et mortalité) chez les patientes et patients sous IPP était légèrement plus élevé que chez les non-utilisateurs (10,6 % c. 10,24 %), et dépendait principalement du taux plus élevé de cas de pneumonie chez les utilisateurs d’IPP (4,0 % c. 3,7 %). On a noté un taux moindre de saignements gastro-intestinaux chez les utilisateurs (1,6 % c. 1,8 %). Le risque de pneumonie était plus marqué dans le sous-groupe soumis à une arthroplastie de la hanche ou du genou (rapport des cotes 1,21, intervalle de confiance de 95 % 1,08–1,36; p = 0,001). On n’a noté aucune différence significative entre les groupes en ce qui concerne la colite à C. difficile ou l’insuffisance rénale aiguë.
Conclusion:: Nous avons constaté que l’utilisation d’IPP préopératoire en période préopératoire était associée aux taux les plus élevés de pneumonie, particulièrement chez la patientèle soumise à une arthroplastie de la hanche ou du genou et à des taux moindres de saignements gastro-intestinaux. Pour la patientèle traitée par IPP avant leur intervention, il faudrait prévoir des mesures afin de réduire le risque de pneumonie, comme la physiothérapie respiratoire, après l’opération.
© 2025 CMA Impact Inc. or its licensors.
Conflict of interest statement
Competing interests:: Kelly Vogt is an associate editor of CJS; she was not involved in the review or decision to accept this manuscript for publication. No other competing interests were declared.
Figures
Similar articles
-
Pharmacological interventions for the prevention of bleeding in people undergoing elective hip or knee surgery: a systematic review and network meta-analysis.Cochrane Database Syst Rev. 2024 Jan 16;1(1):CD013295. doi: 10.1002/14651858.CD013295.pub2. Cochrane Database Syst Rev. 2024. PMID: 38226724 Free PMC article.
-
Proton pump inhibitors for the prevention of non-steroidal anti-inflammatory drug-induced ulcers and dyspepsia.Cochrane Database Syst Rev. 2025 May 8;5(5):CD014585. doi: 10.1002/14651858.CD014585.pub2. Cochrane Database Syst Rev. 2025. PMID: 40337979
-
What Are the Recurrence Rates, Complications, and Functional Outcomes After Multiportal Arthroscopic Synovectomy for Patients With Knee Diffuse-type Tenosynovial Giant-cell Tumors?Clin Orthop Relat Res. 2024 Jul 1;482(7):1218-1229. doi: 10.1097/CORR.0000000000002934. Epub 2023 Dec 28. Clin Orthop Relat Res. 2024. PMID: 38153106 Free PMC article.
-
Does Augmenting Irradiated Autografts With Free Vascularized Fibula Graft in Patients With Bone Loss From a Malignant Tumor Achieve Union, Function, and Complication Rate Comparably to Patients Without Bone Loss and Augmentation When Reconstructing Intercalary Resections in the Lower Extremity?Clin Orthop Relat Res. 2025 Jun 26. doi: 10.1097/CORR.0000000000003599. Online ahead of print. Clin Orthop Relat Res. 2025. PMID: 40569278
-
Association Between Preoperative Anemia and Cognitive Function in a Large Cohort Study of Older Patients Undergoing Elective Surgery.Anesth Analg. 2025 Jan 1;140(1):14-23. doi: 10.1213/ANE.0000000000006998. Epub 2024 Jul 10. Anesth Analg. 2025. PMID: 38985884
References
-
- Abrahami D, McDonald EG, Schnitzer M, et al. Trends in prescribing patterns of proton pump inhibitors surrounding new guidelines. Ann Epidemiol 2021;55:24–6. - PubMed
-
- Canadian Institute for Health Information. Drug use among seniors in Canada, 2016. Ottawa: CIHI; 2018.
-
- Alhazzani W, Alenezi F, Jaeschke RZ, et al. Proton pump inhibitors versus histamine 2 receptor antagonists for stress ulcer prophylaxis in critically ill patients: a systematic review and meta-analysis. Crit Care Med 2013;41:693–705. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical