

Age-dependent phenotypic and molecular evolution of pediatric MDS arising from GATA2 deficiency
- PMID: 40664679
- PMCID: PMC12264048
- DOI: 10.1038/s41408-025-01309-6
Age-dependent phenotypic and molecular evolution of pediatric MDS arising from GATA2 deficiency
Abstract
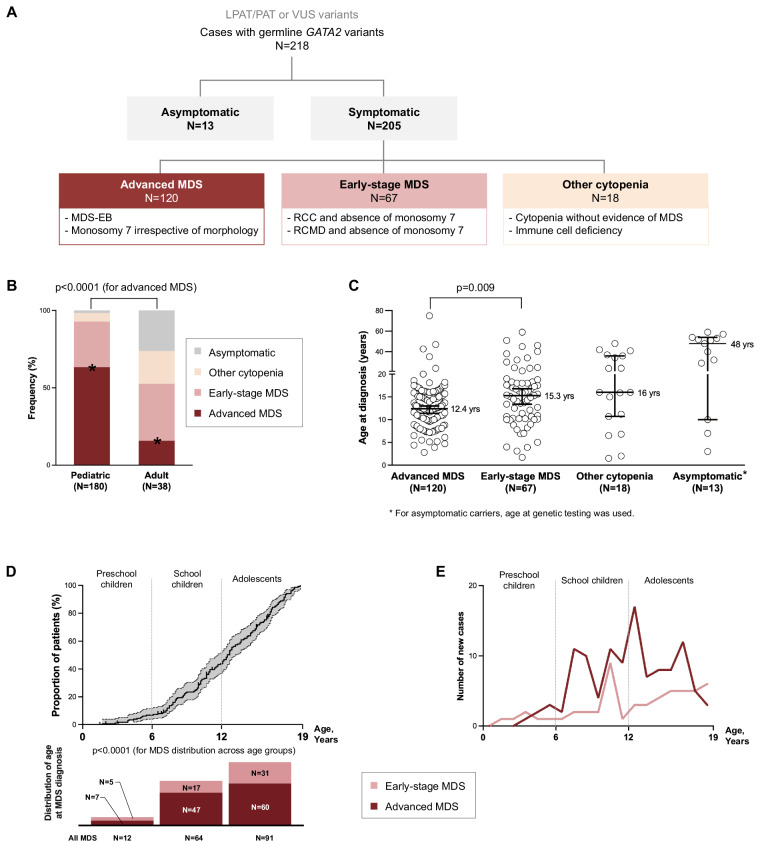
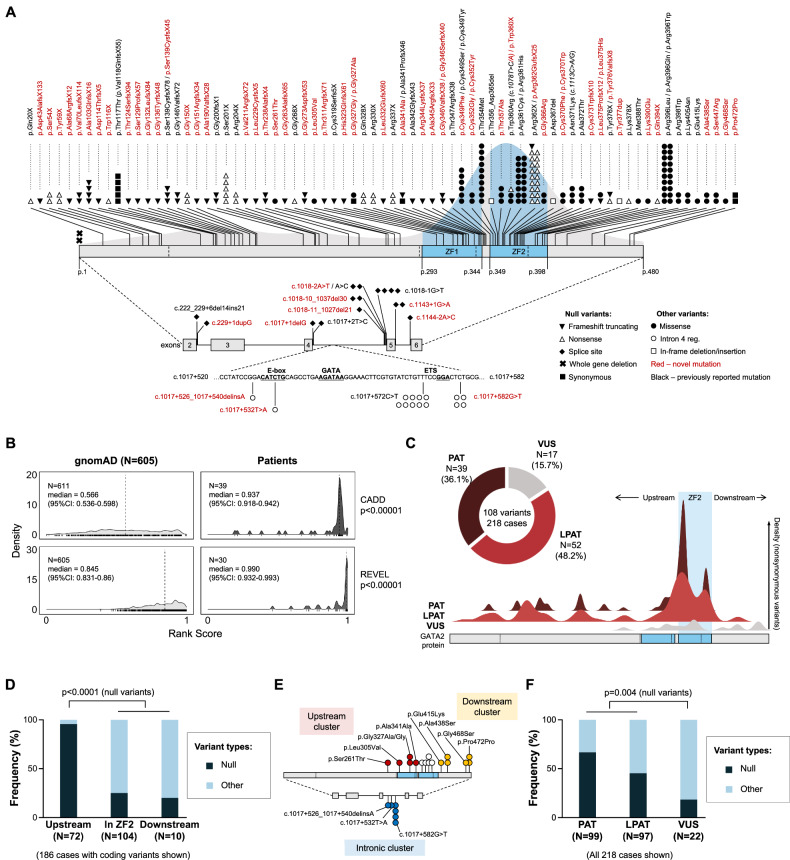
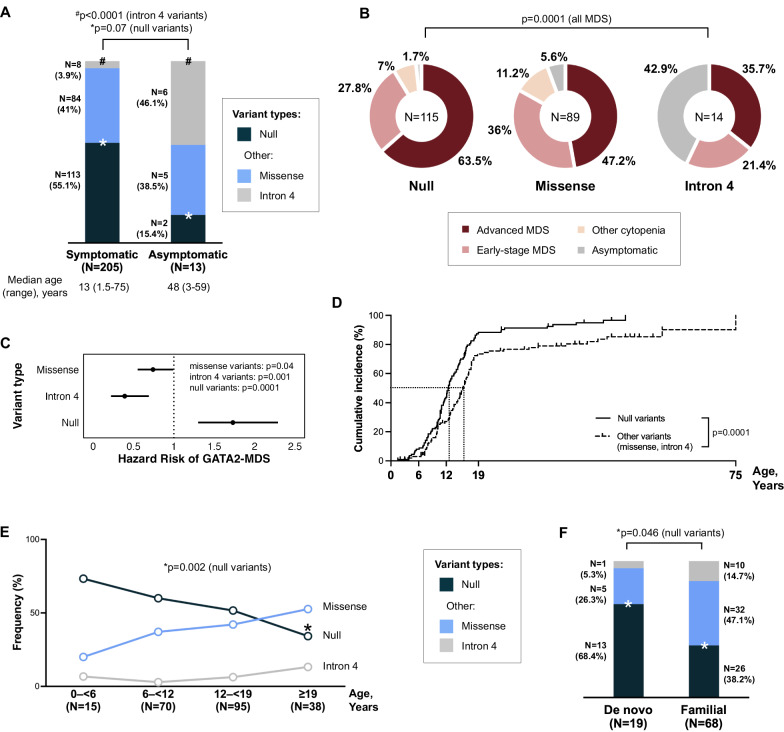
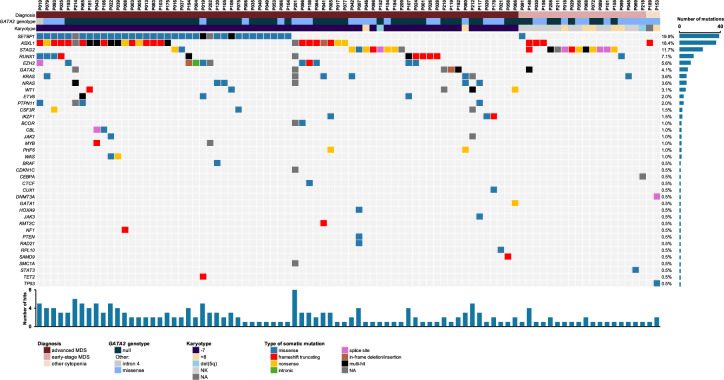
GATA2 deficiency is an autosomal dominant transcriptopathy disorder with high risk for myelodysplastic syndrome (MDS). To elucidate genotype-phenotype associations and identify new genetic risk factors for MDS, we analyzed 218 individuals with germline heterozygous GATA2 variants. We observed striking age-dependent incidence patterns in GATA2-related MDS (GATA2-MDS), with MDS being absent in infants, rare before age 6 years, and steeply increasing in older children. Among 108 distinct GATA2 variants (67 novel), null mutations conferred a 1.7-fold increased risk for MDS, had earlier MDS onset compared to other variants (12.2 vs. 14.6 years, p = 0.009) and were associated with lymphedema and deafness. In contrast, intron 4 variants exhibited reduced penetrance and lower risk for MDS development. Analysis of the somatic landscape revealed unique patterns of clonal hematopoiesis. SETBP1 mutations occurred exclusively in patients with monosomy 7 and their frequency decreased with age. Conversely, the frequency of STAG2 mutations and trisomy 8 increased with age and appeared protective against early development of advanced MDS. Overall, the majority (73.9%) of mutation-positive cases harbored monosomy 7, suggesting it serves as a major driver in malignant progression. Our findings provide evidence for age-appropriate surveillance, and a foundation for genotype-driven risk stratification in GATA2 deficiency.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: Claudia Wehr: honoraria from Takeda, Grifols, Jazz Pharmaceuticals and MSD (not related to the work in this manuscript). Marcin Wlodarski: Retro bio, Guidepoint and OLG Research & Consulting (consultancy) not related to the work in this manuscript.
Figures

References
-
- Ostergaard P, Simpson MA, Connell FC, Steward CG, Brice G, Woollard WJ et al. Mutations in GATA2 cause primary lymphedema associated with a predisposition to acute myeloid leukemia (Emberger syndrome). Nat Genet. 2011;43:929–31. - PubMed
-
- Hirabayashi S, Wlodarski MW, Kozyra E, Niemeyer CM. Heterogeneity of GATA2-related myeloid neoplasms. Int J Hematol. 2017;106:175–82. - PubMed
MeSH terms
Substances
Grants and funding
- 5P30CA021765/U.S. Department of Health & Human Services | NIH | NCI | Division of Cancer Epidemiology and Genetics, National Cancer Institute (National Cancer Institute Division of Cancer Epidemiology and Genetics)
- Advanced Momentum Grant/Magyar Tudományos Akadémia (Hungarian Academy of Sciences)
- Research Mobility Grant 2023/European Hematology Association (EHA)
- 228/C/2020/Fundació la Marató de TV3 (TV3 Marathon Foundation)
- K99 DK135910/DK/NIDDK NIH HHS/United States
- P30 CA021765/CA/NCI NIH HHS/United States
- H2020-739593/EC | Horizon 2020 Framework Programme (EU Framework Programme for Research and Innovation H2020)
- AC23_2/00040/Ministry of Economy and Competitiveness | Instituto de Salud Carlos III (Institute of Health Carlos III)
- 202001-32/Fundació la Marató de TV3 (TV3 Marathon Foundation)
- 1K99DK135910-01A1/U.S. Department of Health & Human Services | NIH | NCI | Division of Cancer Epidemiology and Genetics, National Cancer Institute (National Cancer Institute Division of Cancer Epidemiology and Genetics)
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
