

APOE ε4 carriers share immune-related proteomic changes across neurodegenerative diseases
- PMID: 40665049
- PMCID: PMC12353839
- DOI: 10.1038/s41591-025-03835-z
APOE ε4 carriers share immune-related proteomic changes across neurodegenerative diseases
Abstract
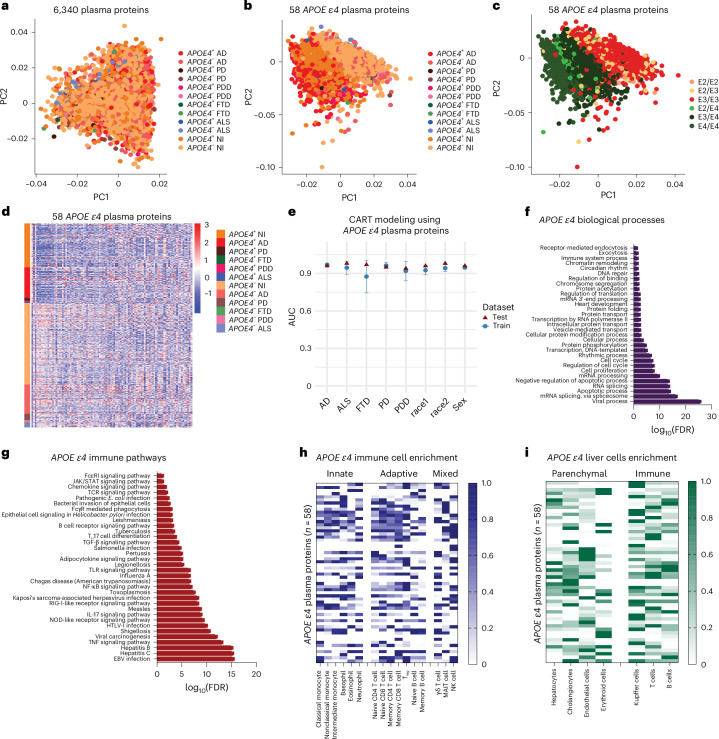
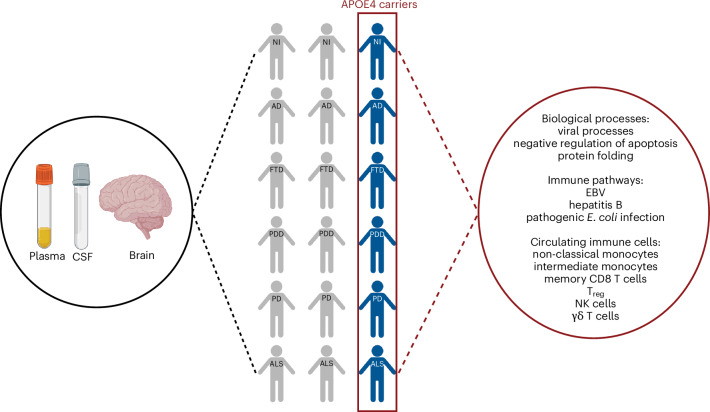
The APOE ε4 genetic variant is the strongest genetic risk factor for late-onset Alzheimer's disease (AD) and is increasingly being implicated in other neurodegenerative diseases. Using the Global Neurodegeneration Proteomics Consortium SomaScan dataset covering 1,346 cerebrospinal fluid (CSF) and 9,924 plasma samples, we used machine learning-based proteome profiling to identify an APOE ε4 proteomic signature shared across individuals with AD, frontotemporal dementia (FTD), Parkinson's disease dementia (PDD), Parkinson's disease (PD), amyotrophic lateral sclerosis (ALS) and nonimpaired controls. This signature was enriched in pro-inflammatory immune and infection pathways as well as immune cells, including monocytes, T cells and natural killer cells. Analysis of the dorsolateral prefrontal cortex proteome for 262 donors from the Accelerating Medicines Partnership for AD UPenn Proteomics Study revealed a consistent APOE ε4 phenotype, independent of neurodegenerative pathology, including amyloid-β tau and gliosis for all diseases, as well as TDP-43 in ALS and FTD cases, and α-synuclein in PD and PDD cases. While systemic proteomic changes were consistent across APOE ε4 carriers, their relationship with clinical and lifestyle factors, such as hypertension and smoking, varied by disease. These findings suggest APOE ε4 confers a systemic biological vulnerability that is necessary but not sufficient for neurodegeneration, emphasizing the need to consider gene-environment interactions. Overall, our study reveals a conserved APOE ε4-associated pro-inflammatory immune signature persistent across the brain, CSF and plasma irrespective of neurodegenerative disease, highlighting a fundamental, disease-independent biological vulnerability to neurodegeneration. This work reframes APOE ε4 as a pleiotropic immune modulator rather than an AD-specific risk gene, providing a foundation for precision biomarker development and early intervention strategies across neurodegenerative diseases.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures







References
-
- Fabre, S. F. et al. Clinic-based cases with frontotemporal dementia show increased cerebrospinal fluid tau and high apolipoprotein E ε4 frequency, but no tau gene mutations. Exp. Neurol.168, 413–418 (2001). - PubMed
-
- Bernardi, L. et al. The effects of APOE and tau gene variability on risk of frontotemporal dementia. Neurobiol. Aging27, 702–709 (2006). - PubMed
-
- Rubino, E. et al. Apolipoprotein E polymorphisms in frontotemporal lobar degeneration: a meta-analysis. Alzheimer’s Dement.9, 706–713 (2013). - PubMed
MeSH terms
Substances
Grants and funding
- R21TR003589/U.S. Department of Health & Human Services | National Institutes of Health (NIH)
- R01AG064227/U.S. Department of Health & Human Services | National Institutes of Health (NIH)
- R01 AG053960/AG/NIA NIH HHS/United States
- R01 AG089497/AG/NIA NIH HHS/United States
- P50AG025688/U.S. Department of Health & Human Services | National Institutes of Health (NIH)
- U01 AG061357/AG/NIA NIH HHS/United States
- R35 NS132179/NS/NINDS NIH HHS/United States
- P50 AG025688/AG/NIA NIH HHS/United States
- 23AARG-1023/ALZ/Alzheimer's Association/United States
- MRF2040081/Department of Health | National Health and Medical Research Council (NHMRC)
- R21 TR003589/TR/NCATS NIH HHS/United States
- R01AG089497/U.S. Department of Health & Human Services | National Institutes of Health (NIH)
- R35NS132179/U.S. Department of Health & Human Services | National Institutes of Health (NIH)
- R01 AG057339/AG/NIA NIH HHS/United States
- RF1 AG057471/AG/NIA NIH HHS/United States
- R01 AG061800/AG/NIA NIH HHS/United States
- U19 AG068054/AG/NIA NIH HHS/United States
- R01 AG057911/AG/NIA NIH HHS/United States
- U19AG068054/U.S. Department of Health & Human Services | National Institutes of Health (NIH)
- P30 AG072973/AG/NIA NIH HHS/United States
- P30AG072973/U.S. Department of Health & Human Services | National Institutes of Health (NIH)
- R01AG07816/U.S. Department of Health & Human Services | National Institutes of Health (NIH)
- U01 AG046161/AG/NIA NIH HHS/United States
- K08AG08604/U.S. Department of Health & Human Services | National Institutes of Health (NIH)
- R01 AG064227/AG/NIA NIH HHS/United States
- RF1 AG057470/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
