

Glenoid morphology in patients undergoing reverse total shoulder arthroplasty due to fracture
- PMID: 40665129
- PMCID: PMC12263477
- DOI: 10.1007/s00402-025-05977-8
Glenoid morphology in patients undergoing reverse total shoulder arthroplasty due to fracture
Abstract
Introduction: Glenoid morphology in patients undergoing reverse total shoulder arthroplasty (rTSA) due to arthritis has been previously studied; however, it has not been as thoroughly evaluated in fracture populations. The purpose of this study is to utilize pre-operative computed tomography (CT) scans to better understand the glenoid anatomy of those patients undergoing rTSA due to fracture.
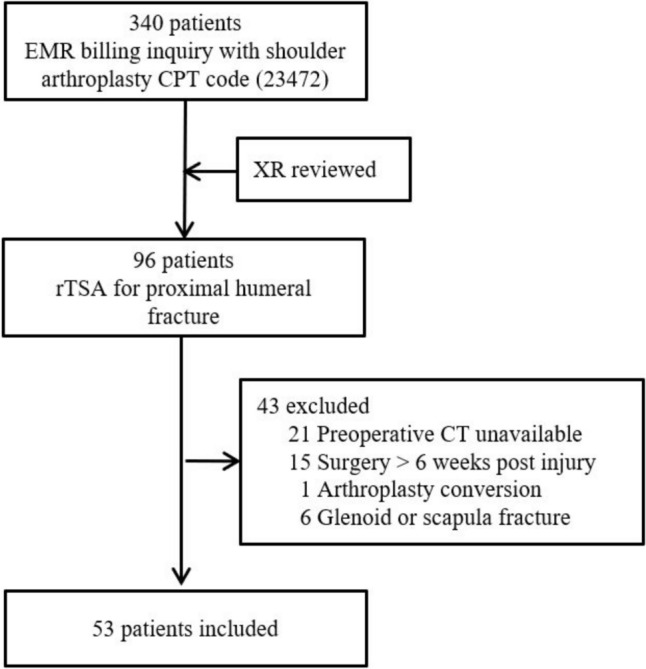
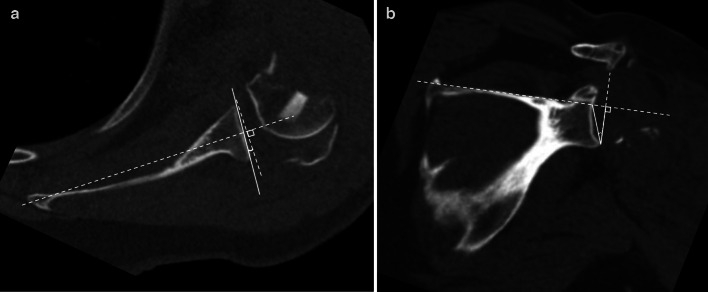
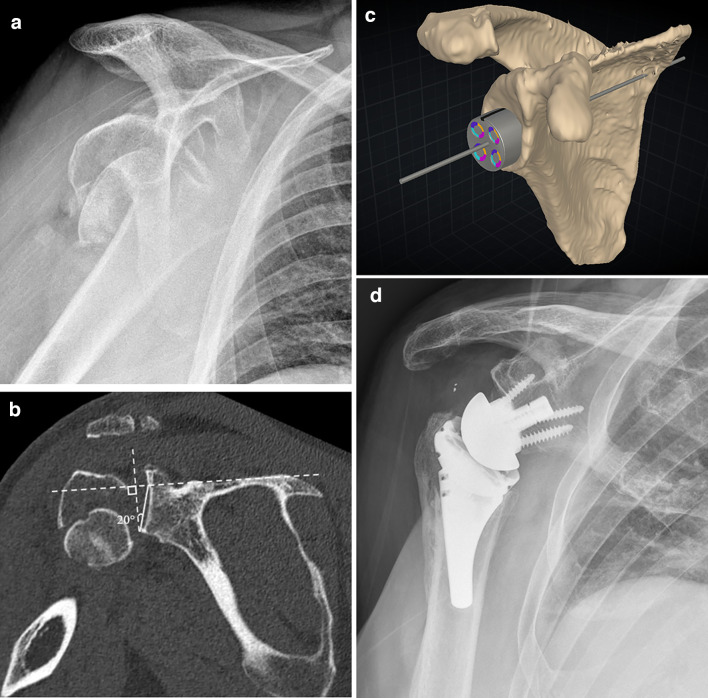
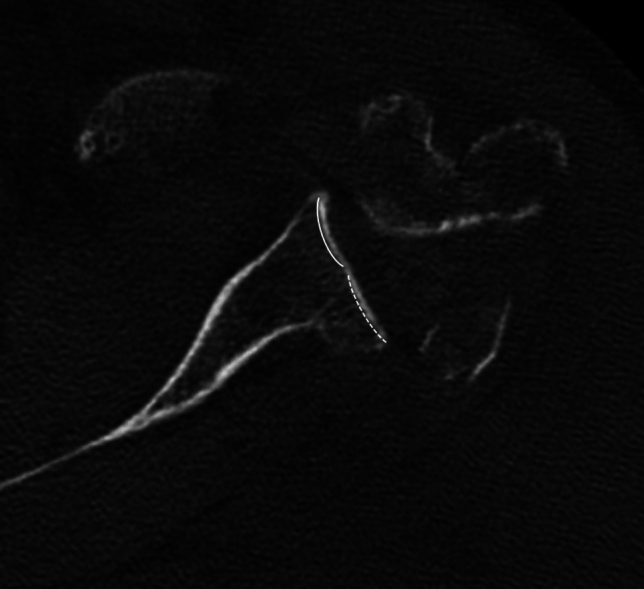
Materials and methods: Patients over the age of 18 who underwent rTSA for proximal humerus fractures from January 1, 2015 to October 31, 2023 at two university health system affiliated hospitals were included if they had a CT scan available for review and image reconstruction. Patients were excluded if a pathologic fracture was identified, surgery was performed greater than 6 weeks after the initial injury, surgery was a conversion or revision surgery, or if a glenoid fracture was present. Glenoid version and reverse shoulder arthroplasty (RSA) angles were measured by a musculoskeletal fellowship-trained radiologist and a shoulder and elbow fellowship-trained orthopaedic surgeon and averaged for final values. Glenoid morphologies were determined using the Walch and Favard classifications.
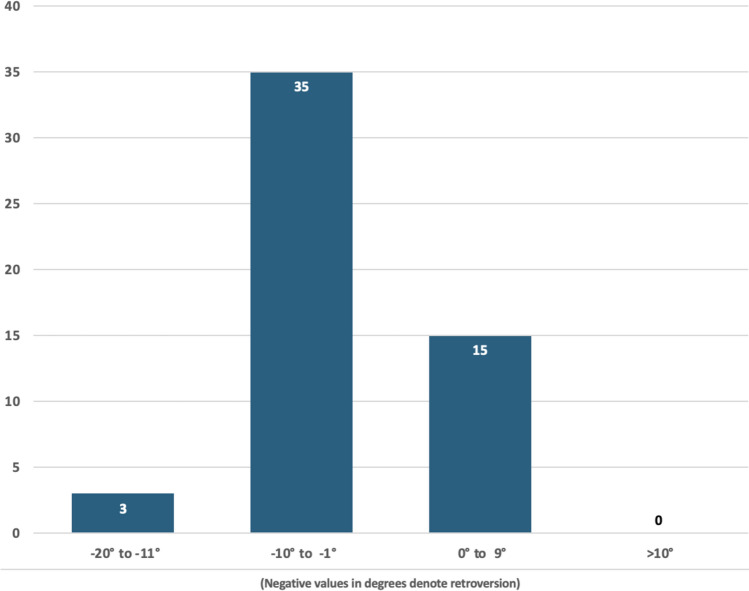
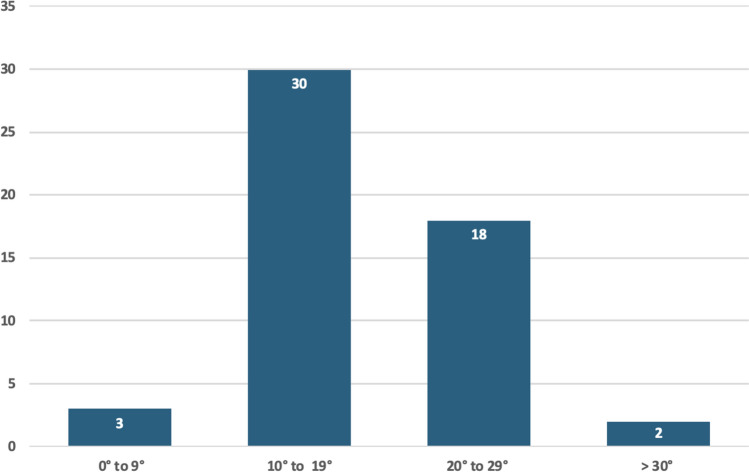
Results: A total of 53 patients with a mean age of 70.4 years (range 36.6-91.2) were included in this study, 84.9% of which were female. Walch A1 glenoid morphology was noted in 92.5% of patients, and Favard E0 morphology was present in 98.1% of patients. Median glenoid version was 3° of retroversion. Median RSA angle was 19°. Of note, 37.7% of patients had a RSA angle of ≥ 20°.
Conclusions: Patients undergoing rTSA for fracture may not have significant glenoid deformity from arthritic wear. However, surgeons should be aware of variations in glenoid version and RSA angle. In this study population, over one-third of patients had a RSA angle of ≥ 20°. Thus, surgeons should take these findings into account when performing rTSA for fracture.
Keywords: Computed tomography; Glenoid anatomy; RSA angle; Reverse total shoulder arthroplasty; Trauma.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: Jackson Hamersly: None Mason Tippy: None James Slaven: None Yohan Jang: Payments (AO Trauma North America, Orthopaedic Trauma Association) Lauren Ladd: Committee/Panel Member (Skeletal Society of Radiology, Radiologic Society of North America, American Association for Women Radiologists, Indiana Radiologic Society) Mark Dillon: Educational Grants (Depuy Synthes), Paid Consultant (Arthrex), Committee Member (American Academy of Orthopaedic Surgeons and American Shoulder and Elbow Surgeons), Stock (ActivArmor).
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
