

Discontinuity of social support among US adults with cognitive impairment before and after the confirmed diagnosis of dementia: a matched ambidirectional cohort study
- PMID: 40665295
- PMCID: PMC12265323
- DOI: 10.1186/s12916-025-04264-y
Discontinuity of social support among US adults with cognitive impairment before and after the confirmed diagnosis of dementia: a matched ambidirectional cohort study
Abstract
Background: Despite increased attention on dementia, much remains unknown about the integration of clinical and non-clinical care, particularly regarding long-term social support, a primary source of non-clinical care. This study uniquely examines the effect of receiving a formal dementia diagnosis on the continuity of social support, an understudied transition point in dementia care pathways.
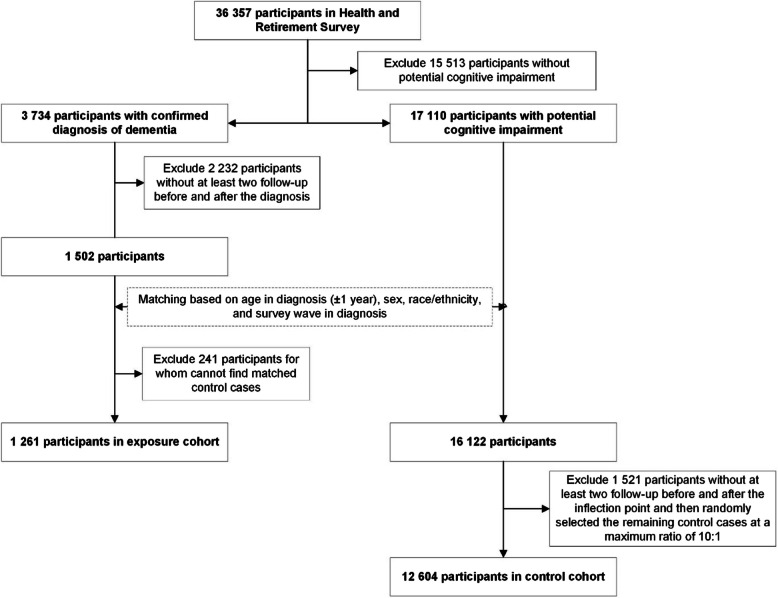
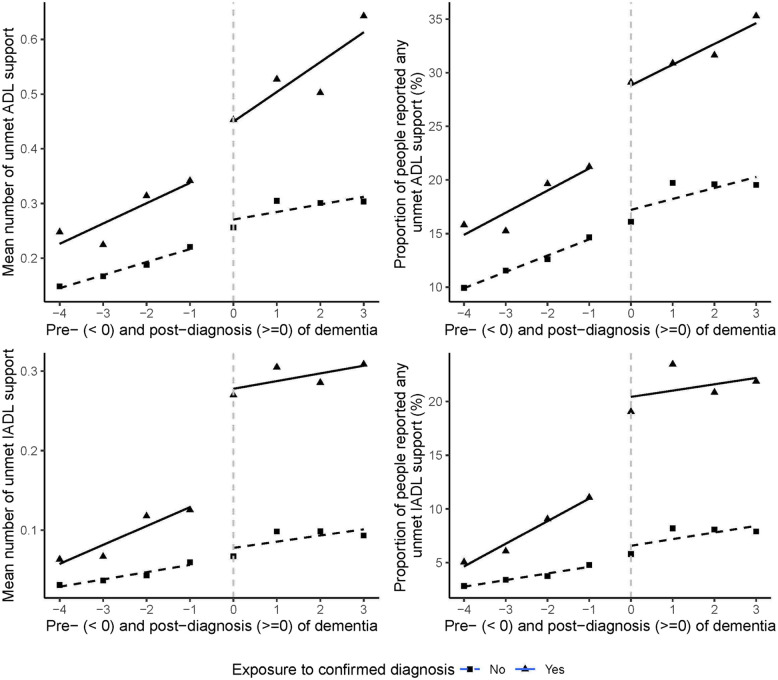
Methods: In this ambidirectional cohort study, we examined ten waves of data from the Health and Retirement Survey(HRS) for US adults over 50 through 2000-2018. Eligibility was limited to participants with cognitive impairment. The exposure group were people with a confirmed dementia diagnosis (N = 1261), and the control group were matched by age, sex, race/ethnicity, and survey wave, but without a confirmed diagnosis (N = 12,604). Unmet social support was defined as reporting physical disability without receiving corresponding social support. Physical disability was assessed using measures of basic activities of daily living (BADLs) and instrumental activities of daily living (IADLs). The data were fitted using controlled interrupted time series analysis to explore the continuity of unmet social support before and after a diagnosis.
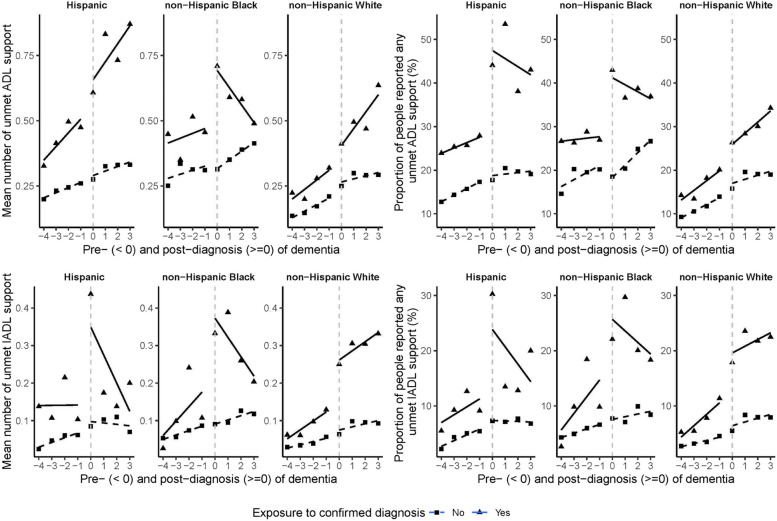
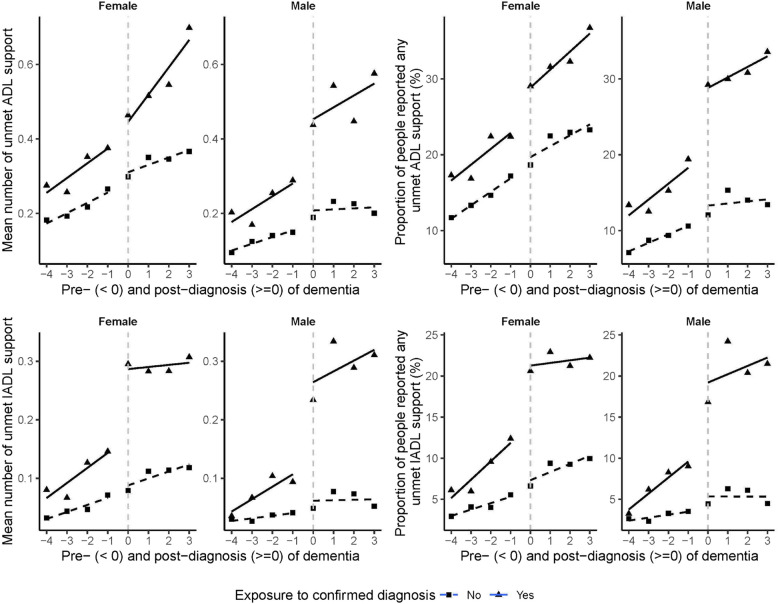
Results: After dementia diagnosis, adults experienced a significant increase in unmet IADL support needs (coef = 0.10, 95% CI [0.07, 0.13]), particularly for making phone calls (coef = 0.74, 95% CI [0.16, 1.33]). By race/ethnicity, Hispanics showed a significant rise in unmet BADL support needs (coef = 0.74, 95% CI [0.03, 1.46]), especially for eating assistance (coef = 1.58, 95% CI [0.17, 2.99]). Blacks experienced increased unmet BADL needs in toileting (coef = 1.52, 95% CI [0.57, 2.47]) and IADL support (coef = 0.09, 95% CI [0.00, 0.17]). Sex disparities were also identified, with females showing decreased unmet BADL support(coef = - 0.55, 95% CI [- 1.03, - 0.06]) but increased unmet IADL support (coef = 0.08, 95% CI [0.04, 0.11]), while males experienced increased unmet toileting (coef = 0.78, 95% CI [0.03, 1.53]) and IADLs support (coef = 0.14, 95% CI [0.10, 0.18]).
Conslusions: Our study identifies a disconnect in the care provided to individuals with dementia before and after their diagnosis. Notably, post-diagnosis, we observed substantial disparities in unmet social support needs across various racial groups. This highlights the need for more cohesive and equitable care strategies in the dementia care continuum.
Keywords: Continuity of care; Dementia; Race/ethnicity; Sex; Social support.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The use of secondary de-identified data makes this study exempt from Institutional Review Board review. All human subjects in the HRS provided informed consent. Consent for publication: Not applicable. Competing interests: BRU is the research and development director at CPFT and elected vice chair of the faculty of old age psychiatry at the Royal College of Psychiatrists. He is the clinical director of the Windsor Unit at Fulbourn Hospital (CPFT), which delivers clinical trials in dementia/mild cognitive impairment for academic and commercial organisations without personal benefit and is the clinical lead for dementia for the NIHR Clinical Research Network (CRN) in the East of England. His lectureship is funded by Gnodde Goldman-Sachs Giving. He has been the principal investigator on trials for Axovant, Pfizer, and EIP Pharma amongst others; his institution has benefited from payment for research carried out but he has not personally received any money. He is a member of an advisory board for Eli Lilly. Other authors declare no conflict of interest with this work.
Figures
Similar articles
-
Occupational therapy for cognitive impairment in stroke patients.Cochrane Database Syst Rev. 2022 Mar 29;3(3):CD006430. doi: 10.1002/14651858.CD006430.pub3. Cochrane Database Syst Rev. 2022. PMID: 35349186 Free PMC article.
-
Clinical judgement by primary care physicians for the diagnosis of all-cause dementia or cognitive impairment in symptomatic people.Cochrane Database Syst Rev. 2022 Jun 16;6(6):CD012558. doi: 10.1002/14651858.CD012558.pub2. Cochrane Database Syst Rev. 2022. PMID: 35709018 Free PMC article.
-
Network Analysis of Key Instrumental Activities of Daily Living and Cognitive Domains for Targeted Intervention in US Older Adults Without Dementia: Cross-Sectional Study.JMIR Aging. 2025 Mar 19;8:e67632. doi: 10.2196/67632. JMIR Aging. 2025. PMID: 40106829 Free PMC article.
-
Racial and ethnic disparities in fecundability: a North American preconception cohort study.Hum Reprod. 2025 Jun 1;40(6):1183-1194. doi: 10.1093/humrep/deaf067. Hum Reprod. 2025. PMID: 40246287
-
Personally tailored activities for improving psychosocial outcomes for people with dementia in long-term care.Cochrane Database Syst Rev. 2018 Feb 13;2(2):CD009812. doi: 10.1002/14651858.CD009812.pub2. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2023 Mar 13;3:CD009812. doi: 10.1002/14651858.CD009812.pub3. PMID: 29438597 Free PMC article. Updated.
References
-
- Arrighi HM, Gelinas I, McLaughlin TP, Buchanan J, Gauthier S. Longitudinal changes in functional disability in Alzheimer’s disease patients. Int Psychogeriatr. 2013;25(6):929–37. - PubMed
-
- World Health Organization: Continuity and coordination of care: a practice brief to support implementation of the WHO Framework on integrated people-centred health services. 2018.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
