

Treatment effects of Xuebijing injection in patients with sepsis by clinical phenotype: a post hoc analysis of the EXIT-SEP trial
- PMID: 40666169
- PMCID: PMC12257024
- DOI: 10.1016/j.eclinm.2025.103341
Treatment effects of Xuebijing injection in patients with sepsis by clinical phenotype: a post hoc analysis of the EXIT-SEP trial
Abstract
Background: Xuebijing injection (XBJ) could improve the outcomes of sepsis patients. However, sepsis is a heterogeneous syndrome, and it remains unclear which patients benefit the most. We aimed to identify the sepsis phenotypes most likely to benefit from XBJ treatment.
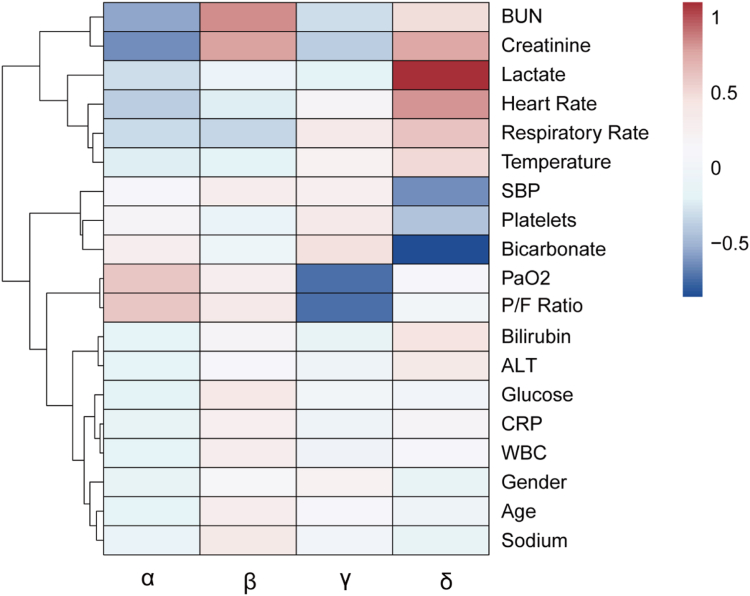
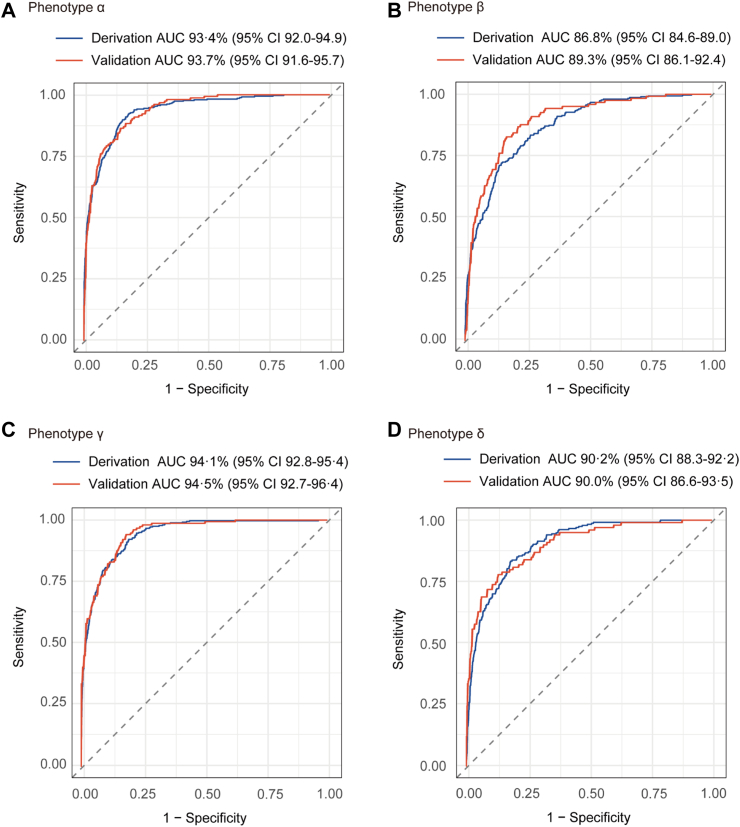
Methods: This post hoc analysis of the EXIT-SEP trial included sepsis patients from 45 intensive care units (ICUs) in China between October 2017 and June 2019. The XBJ group received 100 mL of XBJ every 12 h for 5 days, while the placebo group was given a volume-matched saline. Consensus k-means clustering was performed to reproduce previously identified sepsis phenotypes in relation to the SENECA classification (α, β, γ, and δ) based on 19 variables such as age, sex, temperature, and biochemistry/lab results. Clinical characteristics and outcomes (28-day mortality, ventilator-free days, ICU-free days), as well as the heterogeneity of treatment effects (HTE), were compared between the four different phenotypes and across treatment groups. We also developed a probabilistic model for phenotype assignment and evaluated its performance in derivation and internal validation cohorts. The EXIT-SEP trial is registered with ClinicalTrials.gov (NCT03238742).
Findings: Among 1760 patients (878 in the XBJ group and 882 in the placebo group), four sepsis phenotypes (α: 28.2%, β: 24.0%, γ: 28.9%, and δ: 18.9%) were replicated based on the SENECA classification. Phenotype α had the lowest 28-day mortality. Phenotype β was associated with older age, chronic illness, and renal dysfunction. Phenotype γ was characterized by respiratory dysfunction. Phenotype δ was associated with acidosis, elevated alanine transaminase, coagulation dysfunction, shock, and the highest 28-day mortality (32.5%). Compared with placebo, XBJ treatment was associated with lower 28-day mortality in patients with phenotype γ (p = 0.003) and δ (p = 0.033), while the treatment-by-phenotype interaction was not statistically significant. Additionally, patients with phenotype δ who received XBJ had more ventilator-free days and ICU-free days than those with phenotype α, with p for interaction < 0.001 for both outcomes. Finally, a parsimonious classifier model demonstrated good accuracy in phenotype prediction, with AUROCs of 0.937 (95% CI: 0.916-0.957) for α, 0.893 (0.861-0.924) for β, 0.945 (0.927-0.964) for γ, and 0.900 (0.866-0.935) for δ in the internal validation cohort.
Interpretation: We replicated four sepsis phenotypes in the EXIT-SEP cohort, with patterns similar to previously established phenotypes. XBJ treatment was associated with lower 28-day mortality in patients with phenotypes γ and δ, but these findings require further validation.
Funding: This study was funded by the National Natural Science Foundation of China; Noncommunicable Chronic Diseases-National Science and Technology Major Project; Zhongda Hospital Affiliated to Southeast University, Jiangsu Province High-Level Hospital Construction Funds; Nanjing Technology Development Program; The Pilot Project of the Flagship Hospital of Integrated Traditional Chinese and Western Medicines in Zhongda Hospital affiliated to Southeast University.
Keywords: Heterogeneity of treatment effect; Phenotypes; Sepsis; Xuebijing injection.
© 2025 The Author(s).
Conflict of interest statement
All authors declare no competing interests.
Figures



References
-
- Xie J., Wang H., Kang Y., et al. The epidemiology of sepsis in Chinese ICUs: a national cross-sectional survey. Crit Care Med. 2020;48:e209–e218. - PubMed
-
- Slim M.A., Turgman O., van Vught L.A., et al. Non-conventional immunomodulation in the management of sepsis. Eur J Intern Med. 2024;121:9–16. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
