

Development of a predictive model for recurrence in postoperative glottic laryngeal squamous cell carcinoma patients following adjuvant chemotherapy based on PNI, NLR, and PLR
- PMID: 40667564
- PMCID: PMC12256410
- DOI: 10.62347/CYNY8714
Development of a predictive model for recurrence in postoperative glottic laryngeal squamous cell carcinoma patients following adjuvant chemotherapy based on PNI, NLR, and PLR
Abstract
Objective: To identify key factors influencing postoperative recurrence in patients with glottic laryngeal squamous cell carcinoma (LSCC) and to develop a predictive model incorporating traditional clinicopathological features and novel inflammatory and immune indicators. This model aims to provide a theoretical foundation for individualized prediction of postoperative recurrence risk and support clinical decision-making.
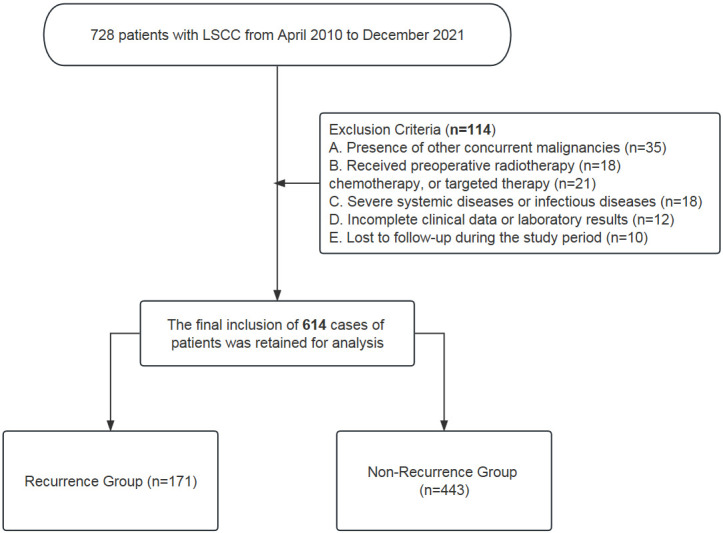
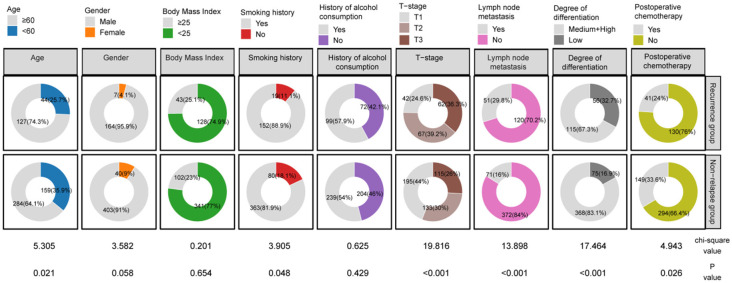
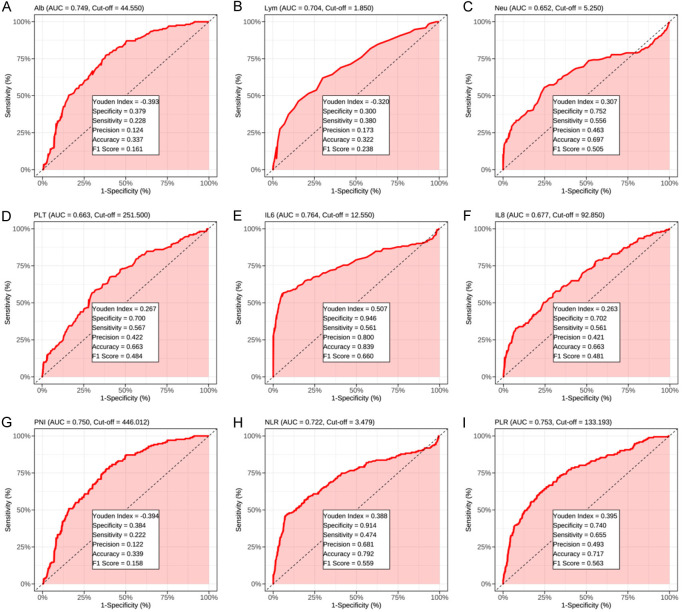
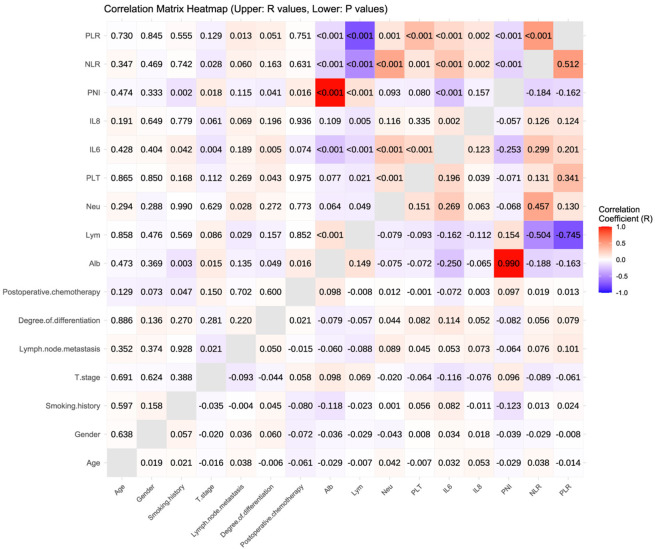
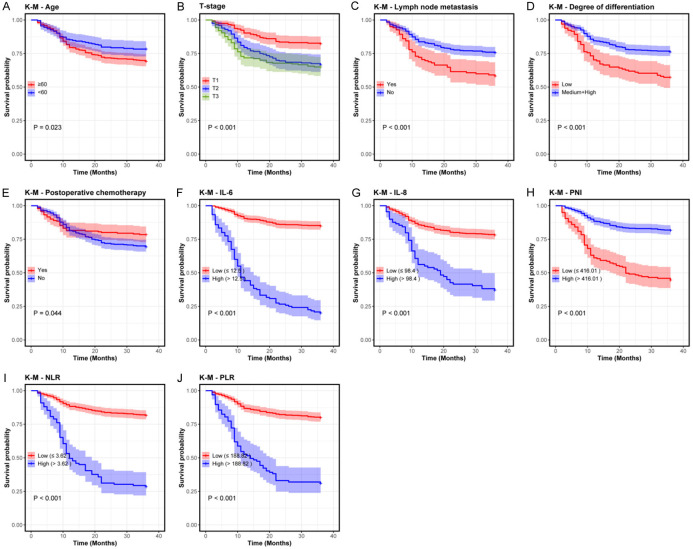
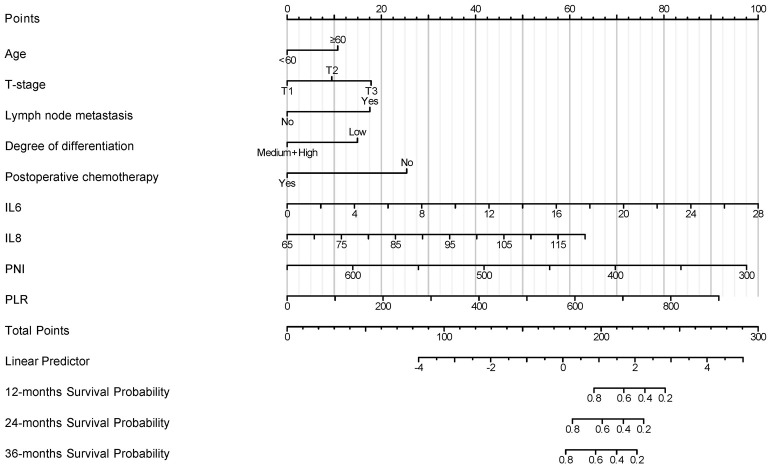
Methods: Clinical and laboratory data were collected from 614 patients with glottic laryngeal cancer who underwent surgery between April 2010 and December 2021. The study included inflammatory and immune-related indicators (such as NLR, PLR, PNI, IL-6, IL-8), alongside traditional clinical features like age, T stage, lymph node metastasis, and degree of differentiation. Univariate and multivariate logistic regression, as well as Cox regression analyses, were performed to identify factors associated with recurrence. A Nomogram model was constructed based on Cox regression results. The model's predictive performance was evaluated using ROC curves, the concordance index (C-index), and calibration curves, with validation conducted in both training and validation cohorts.
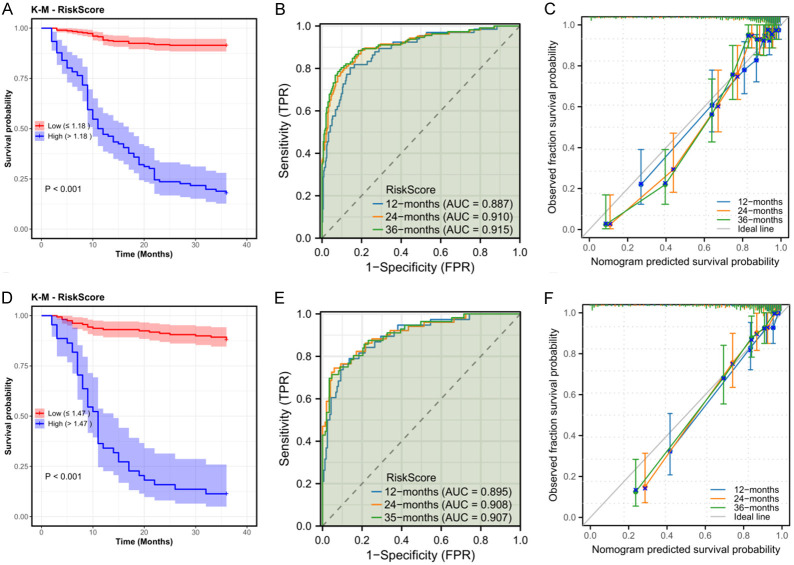
Results: Multivariate analysis identified age, T stage, lymph node metastasis, degree of differentiation, IL-6, IL-8, PNI, and PLR as independent factors influencing postoperative recurrence in patients with glottic laryngeal cancer. The Nomogram model demonstrated excellent predictive performance in both the training and validation cohorts, with AUCs for 12-, 24-, and 36-month recurrence-free survival predictions of 0.887, 0.906, and 0.915 (training cohort) and 0.895, 0.906, and 0.907 (validation cohort), respectively. The model's concordance indices were 0.860 and 0.857 in the training and validation groups, respectively. Calibration curves revealed a high degree of agreement between predicted and actual outcomes.
Conclusion: The Nomogram model developed in this study integrates multiple clinical and inflammatory-immune indicators, enabling accurate prediction of 12-, 24-, and 36-month recurrence-free survival rates in post-surgical patients with glottic laryngeal cancer. The model holds significant clinical value, with IL-6, IL-8, and PNI identified as crucial indicators for predicting recurrence risk, providing valuable insights for postoperative follow-up and individualized treatment strategies.
Keywords: Glottic laryngeal cancer; inflammatory markers; nomogram model; postoperative recurrence; prognostic nutritional index (PNI).
AJCR Copyright © 2025.
Conflict of interest statement
None.
Figures
References
-
- Cavaliere M, Bisogno A, Scarpa A, D’Urso A, Marra P, Colacurcio V, De Luca P, Ralli M, Cassandro E, Cassandro C. Biomarkers of laryngeal squamous cell carcinoma: a review. Ann Diagn Pathol. 2021;54:151787. - PubMed
-
- Yanes M, Santoni G, Maret-Ouda J, Ness-Jensen E, Färkkilä M, Lynge E, Pukkala E, Romundstad P, Tryggvadóttir L, Euler-Chelpin MV, Lagergren J. Laryngeal and pharyngeal squamous cell carcinoma after antireflux surgery in the 5 nordic countries. Ann Surg. 2022;276:e79–e85. - PubMed
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous