

Clinical heterogeneity and phenotyping of post cardiac arrest brain injury: one size may not fit all
- PMID: 40668231
- PMCID: PMC12283859
- DOI: 10.1007/s00134-025-08012-x
Clinical heterogeneity and phenotyping of post cardiac arrest brain injury: one size may not fit all
Abstract
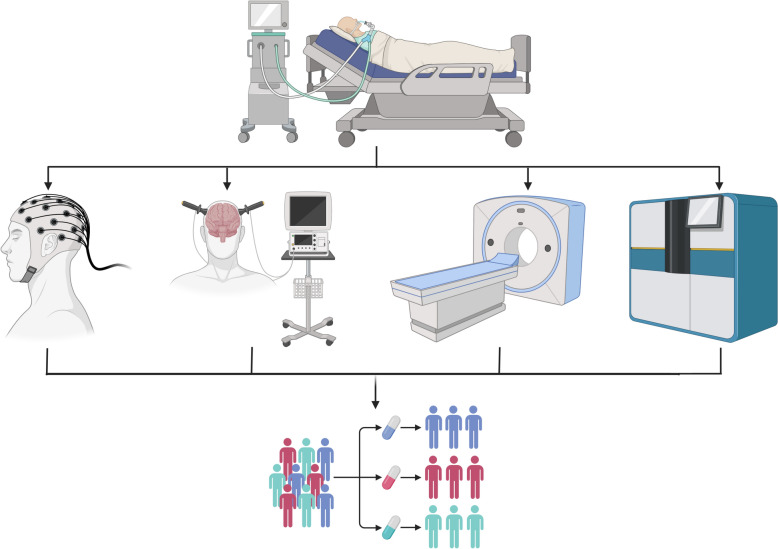
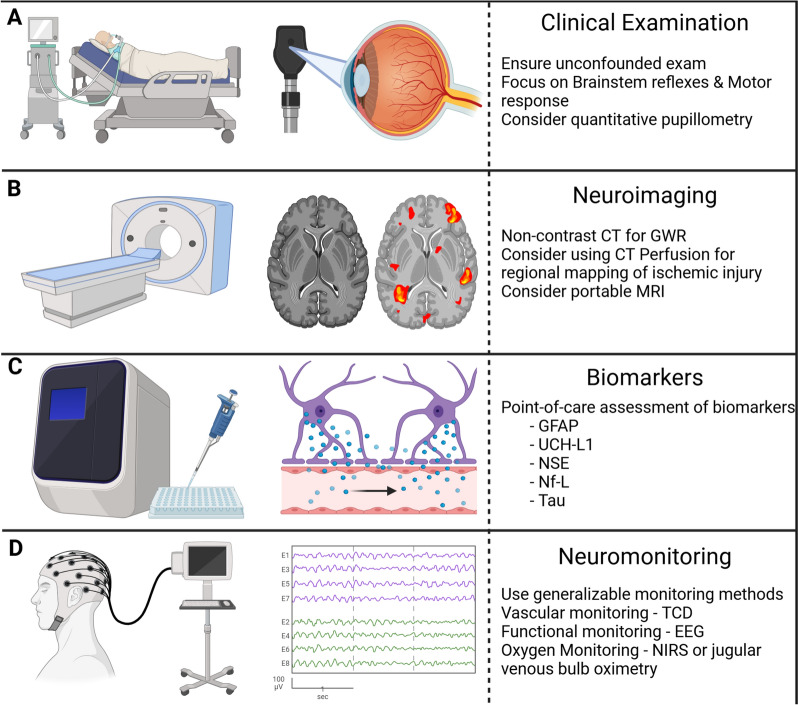
Post-cardiac arrest brain injury (PCABI) emanates from the injurious pathophysiologic sequelae that take place during and after resuscitation from cardiac arrest. Regrettably, identification of efficacious management strategies to mitigate PCABI has been disappointing with numerous well-conducted randomized control trials yielding neutral results. The reasons for this observation are likely multifactorial, however, increasingly patient and disease-specific heterogeneity is recognized as a crucial factor in clinical decision-making. Traditionally, PCABI has been stratified based upon simple historical characteristics (e.g. location of cardiac arrest, initial rhythm, witnessed vs. unwitnessed) that inadequately reflect in vivo PCABI severity or responses to clinical interventions within individual patients. It is therefore increasingly clear that this approach to PCABI is insufficient. In other syndromes, such as sepsis or acute respiratory distress syndrome, attempts to identify early "phenotypes" of patients reflect growing recognition of considerable between-patient heterogeneity in the disease mechanisms and response to therapeutic interventions. A similar approach should be taken with PCABI. In this review, we described the clinical heterogeneity and phenotypes of PCABI as related to the underlying pathophysiology, selective anatomical vulnerability and electrographic patterns. The overarching aim of the review is the propose a shift to expeditious phenotyping of PCABI severity that focuses on assessing in vivo severity and patterns of injury that could be used for future targeted therapies. We will also discuss potential causes of heterogeneous clinical responses to interventions and highlight future research areas for PCABI that focus on phenotyping and incorporating these considerations into clinical trials.
Keywords: Cardiac arrest; Heterogeneity; Phenotypes; Post-cardiac arrest brain injury; Return of spontaneous circulation.
© 2025. The Author(s).
Conflict of interest statement
Declaration. Conflicts of interest: CR is Deputy Editor for Intensive Care Medicine. She has not taken part in the review or selection process of this article. All other authors have no conflicts of interest.
Figures
Similar articles
-
Systemic Inflammatory Response Syndrome.2025 Jun 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jun 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 31613449 Free Books & Documents.
-
Hypothermia for neuroprotection in adults after cardiopulmonary resuscitation.Cochrane Database Syst Rev. 2016 Feb 15;2(2):CD004128. doi: 10.1002/14651858.CD004128.pub4. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2023 May 22;5:CD004128. doi: 10.1002/14651858.CD004128.pub5. PMID: 26878327 Free PMC article. Updated.
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Short-Term Memory Impairment.2024 Jun 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Jun 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 31424720 Free Books & Documents.
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.Health Technol Assess. 2006 Sep;10(34):iii-iv, ix-xi, 1-204. doi: 10.3310/hta10340. Health Technol Assess. 2006. PMID: 16959170
References
-
- Neumar RW, Nolan JP, Adrie C et al (2008) Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A consensus statement from the International Liaison Committee on Resuscitation (American Heart Association, Australian and New Zealand Council on Resuscitation, European Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Asia, and the Resuscitation Council of Southern Africa); the American Heart Association Emergency Cardiovascular Care. Circulation 118(23):2452–2483 - PubMed
-
- Bunch TJ, White RD, Gersh BJ et al (2003) Long-term outcomes of out-of-hospital cardiac arrest after successful early defibrillation. N Engl J Med 348(26):2626–2633 - PubMed
-
- Gräsner J-T, Lefering R, Koster RW et al (2016) EuReCa ONE—27 Nations, ONE Europe, ONE Registry A prospective one month analysis of out-of-hospital cardiac arrest outcomes in 27 countries in Europe on behalf of EuReCa ONE Collaborators 1. Resuscitation 105(105):188–195 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
