

Characterising and Evaluating the Immune Microenvironment Landscapes of Colorectal Cancer Shaped by Different Therapies
- PMID: 40669056
- PMCID: PMC12266622
- DOI: 10.1049/syb2.70028
Characterising and Evaluating the Immune Microenvironment Landscapes of Colorectal Cancer Shaped by Different Therapies
Abstract
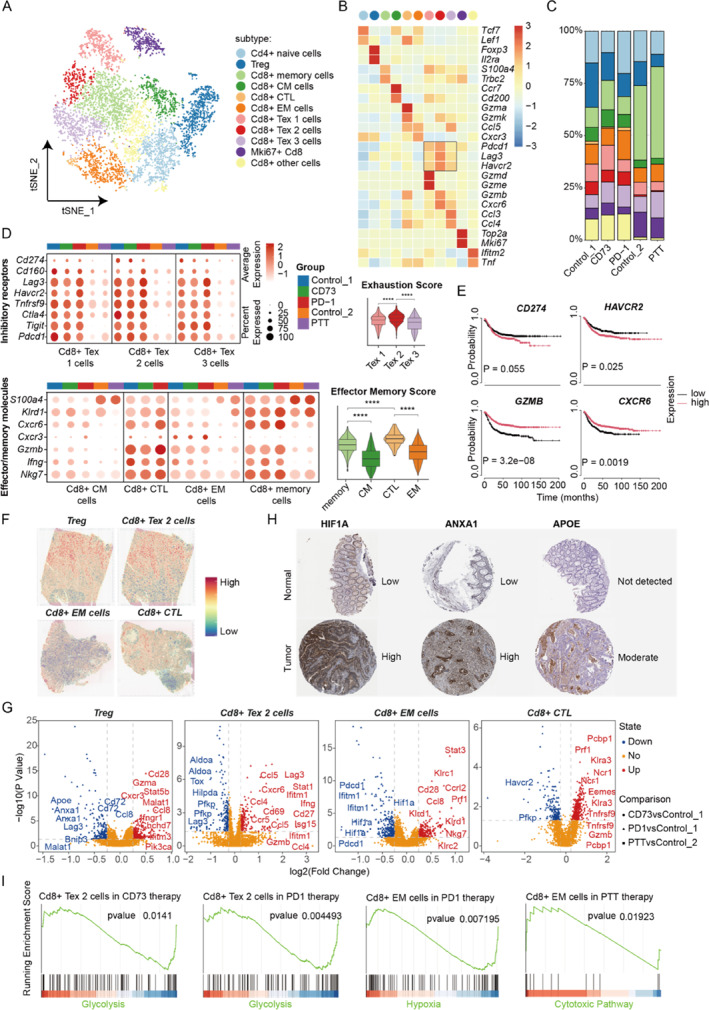
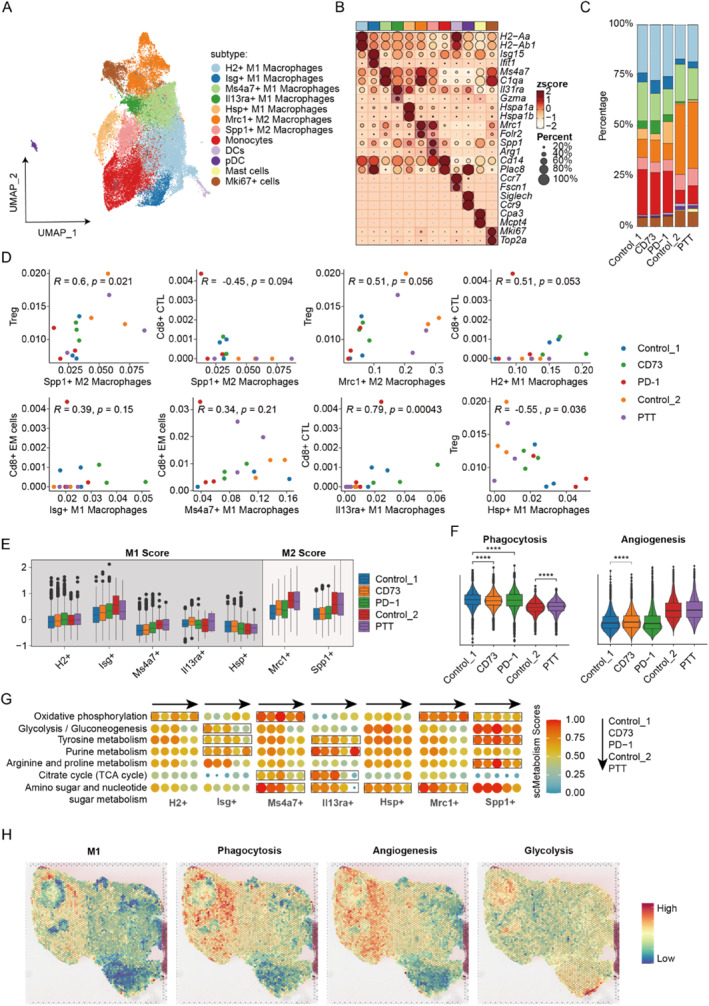
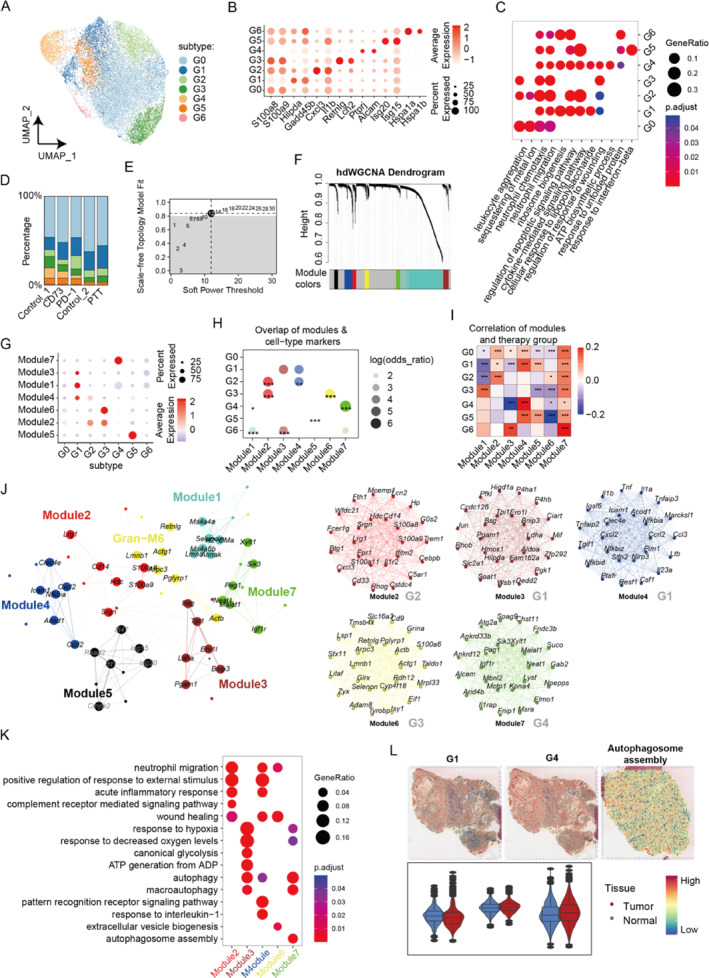
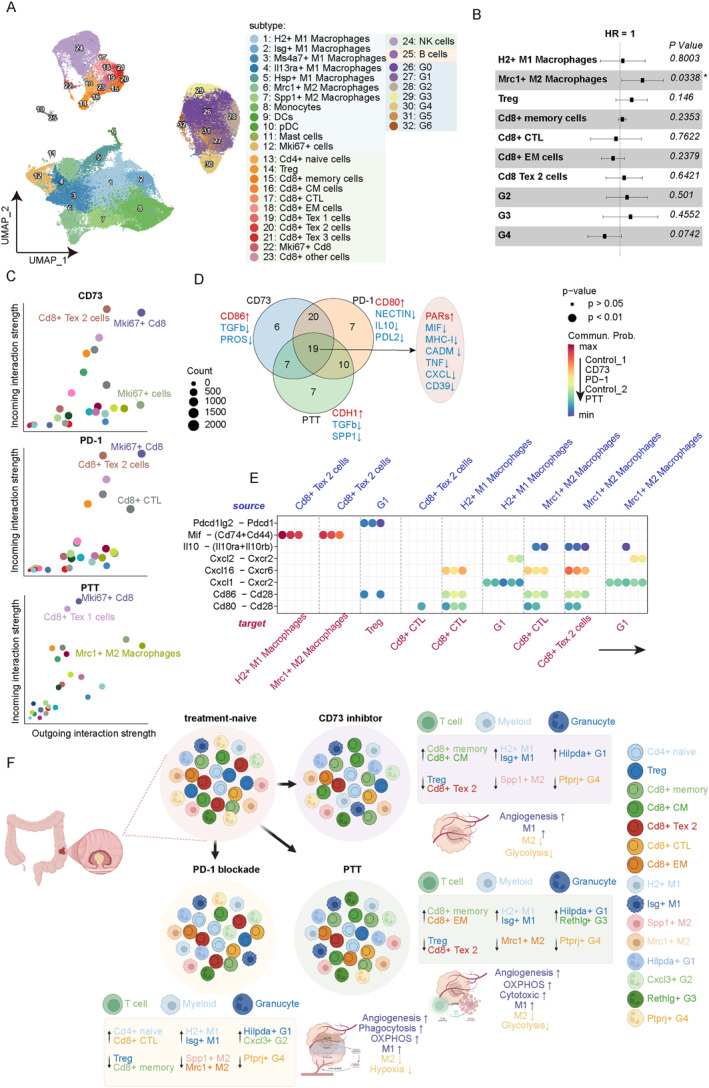
Colorectal cancer (CRC) occurs as the third most common cancer with high mortality across the world. Understanding the intratumoral immune cell heterogeneity and their responses to various therapies is crucial for enhancing patient outcomes. This study aimed to characterise and evaluate the immune microenvironment landscapes of CRC shaped by different therapies including CD73 inhibitor, PD-1 blockade and photothermal therapy (PTT). Our investigation revealed that three therapies could commonly modulate the down-regulation of Treg, M2 macrophage and Ptprj+ G4 granulocyte, up-regulation of effector/memory T cell, M1 macorphage and Hilpda+ G1 granulocyte. Moreover, we identified the uniquely dis-regulated cell types and pathway activities response to each therapy, such as CD73 inhibitor enriched more Cd8+ memory and central memory (CM) cell, PD-1 blockade with more Cd8+ CTL and Cxcl3+ G2 granulocyte, and PTT with more Cd8+ effector memory and Rethlg+ G3 granulocyte cell. These responses disordered the glycolysis, angiogenesis, phagocytosis functions and cellular communication to reshape the CRC tumour immune microenvironment. We provide the detail insights into the intratumoral immunomodulation preferences of CRC mice treated with CD73 inhibitor, PD-1 blockade and PTT therapies, which might contribute to the ongoing development of more effective anticancer strategies.
Keywords: RNA; bioinformatics; cancer; data analysis.
© 2025 The Author(s). IET Systems Biology published by John Wiley & Sons Ltd on behalf of The Institution of Engineering and Technology.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Oncolytic reovirus enhances the effect of CEA immunotherapy when combined with PD1-PDL1 inhibitor in a colorectal cancer model.Immunotherapy. 2025 Apr;17(6):425-435. doi: 10.1080/1750743X.2025.2501926. Epub 2025 May 12. Immunotherapy. 2025. PMID: 40353308
-
SLC4A4 Moulds the Inflammatory Tumor Microenvironment and Predicts Therapeutic Expectations in Colorectal Cancer.Curr Med Chem. 2025;32(19):3861-3878. doi: 10.2174/0109298673277357231218070812. Curr Med Chem. 2025. PMID: 38310390
-
Diversity of mast cell subpopulations in the tumor microenvironment of colorectal cancer and their prognostic implications.Cancer Immunol Immunother. 2025 Jun 30;74(8):255. doi: 10.1007/s00262-025-04119-8. Cancer Immunol Immunother. 2025. PMID: 40586903 Free PMC article.
-
Systemic treatments for metastatic cutaneous melanoma.Cochrane Database Syst Rev. 2018 Feb 6;2(2):CD011123. doi: 10.1002/14651858.CD011123.pub2. Cochrane Database Syst Rev. 2018. PMID: 29405038 Free PMC article.
-
Immunotherapy in microsatellite-stable colorectal cancer: Strategies to overcome resistance.Crit Rev Oncol Hematol. 2025 Aug;212:104775. doi: 10.1016/j.critrevonc.2025.104775. Epub 2025 May 21. Crit Rev Oncol Hematol. 2025. PMID: 40409481 Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
