

Metabolic fingerprinting enables rapid, label-free histopathology in gastric cancer diagnosis and prognostic prediction
- PMID: 40669450
- PMCID: PMC12281434
- DOI: 10.1016/j.xcrm.2025.102238
Metabolic fingerprinting enables rapid, label-free histopathology in gastric cancer diagnosis and prognostic prediction
Abstract
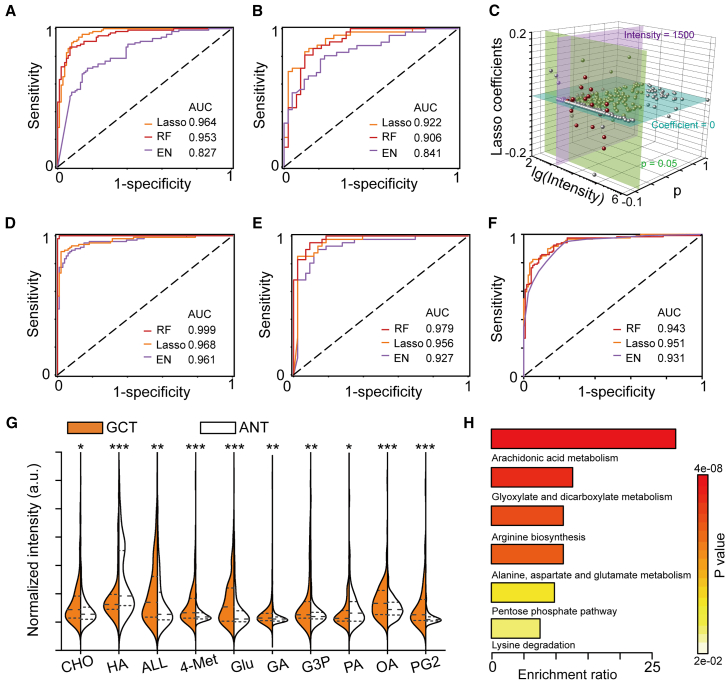
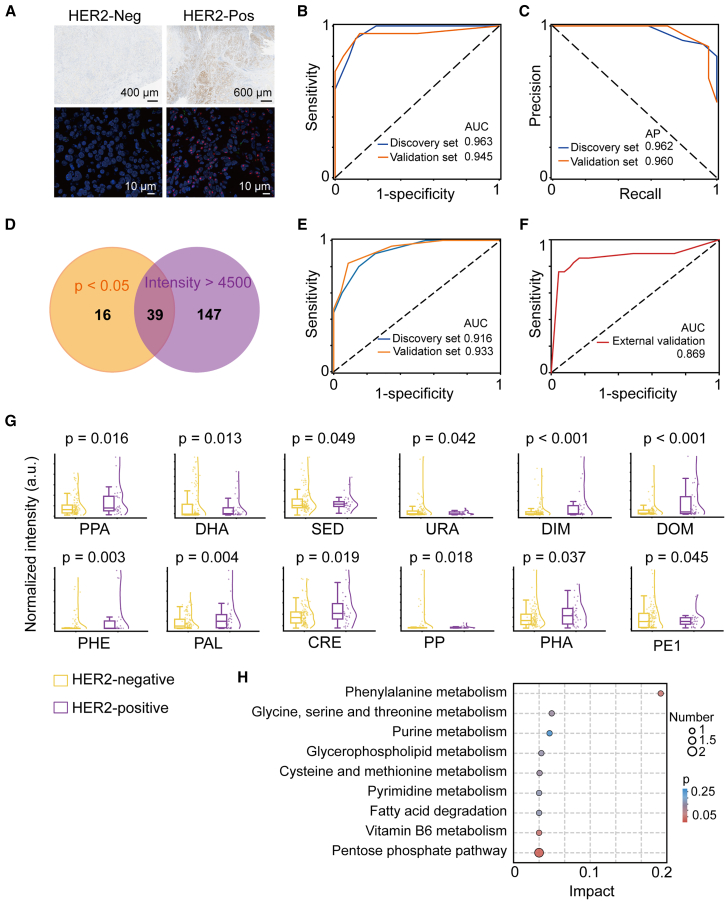
Histopathological evaluation is a cornerstone of cancer identification but often involves time-consuming labeling processes (∼days per sample) and experience-dependent interpretation. Herein, we introduce a rapid (∼40 min per sample) and label-free histopathological method based on metabolic fingerprinting of tissue using nanoparticle-enhanced laser desorption/ionization mass spectrometry. Applied to gastric cancer (GC, n = 284 paired tissue), this approach distinguishes malignant from benign tissues (area under the curve [AUC] of 0.979), identifies tumor subtypes (AUC of 0.963), and assesses prognosis (p < 0.05) without specialized pathologists. External validation on 238 samples from an independent cohort confirmed its robustness. This method advances histopathological analysis, offering potential for scalable clinical use.
Keywords: diagnosis; gastric cancer; metabolic biomarkers; pathology; prognosis; tissue.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare competing financial interests. Both the technology and the method of detecting bio-samples are patented by the authors.
Figures






References
-
- Cubillos-Ruiz A., Guo T., Sokolovska A., Miller P.F., Collins J.J., Lu T.K., Lora J.M. Engineering living therapeutics with synthetic biology. Nat. Rev. Drug Discov. 2021;20:941–960. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
