

Tau PET positivity in individuals with and without cognitive impairment varies with age, amyloid-β status, APOE genotype and sex
- PMID: 40670684
- PMCID: PMC12321570
- DOI: 10.1038/s41593-025-02000-6
Tau PET positivity in individuals with and without cognitive impairment varies with age, amyloid-β status, APOE genotype and sex
Abstract
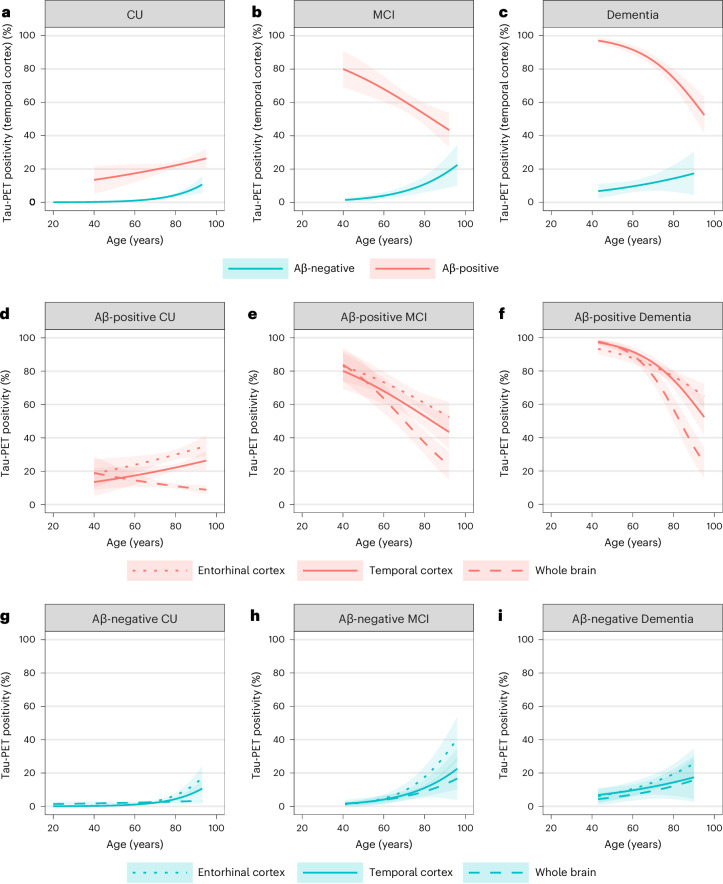
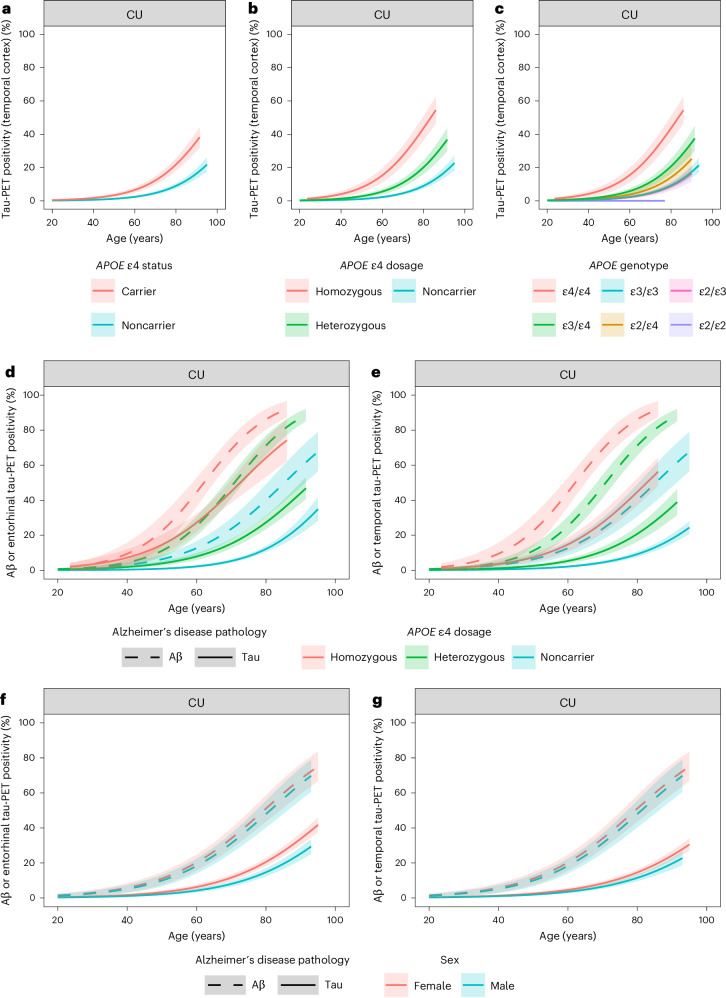
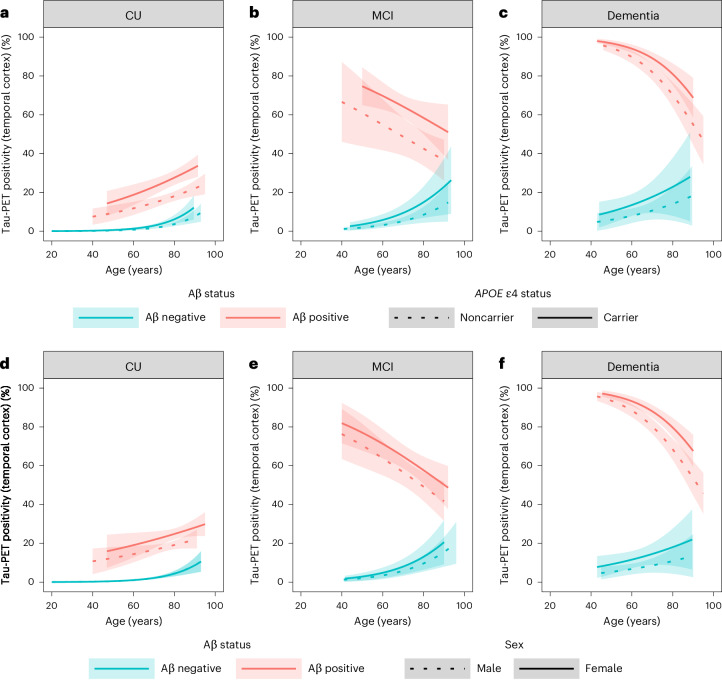
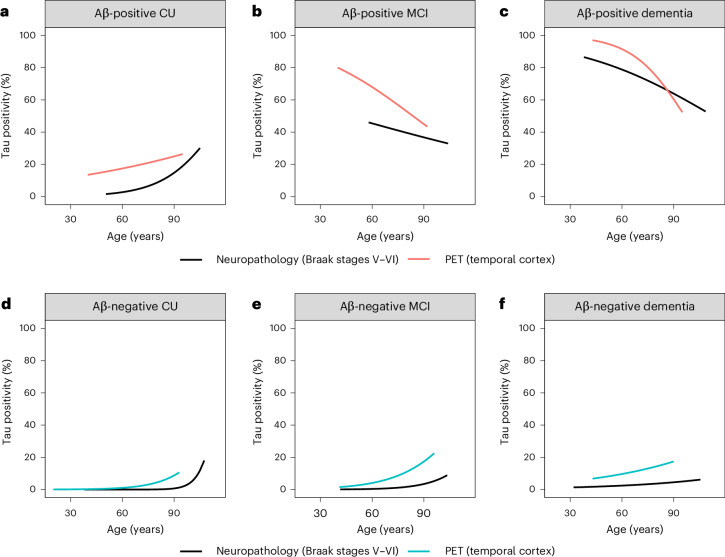
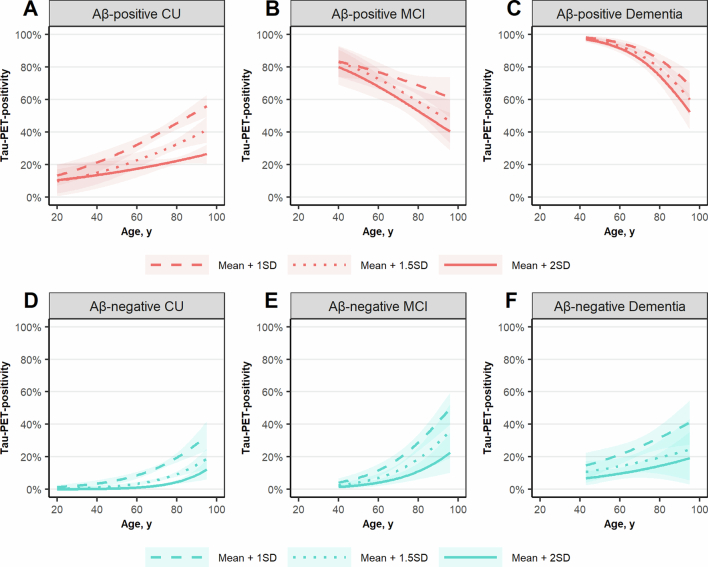
Tau positron emission tomography (PET) imaging allows in vivo detection of tau proteinopathy in Alzheimer's disease, which is associated with neurodegeneration and cognitive decline. Understanding how demographic, clinical and genetic factors relate to tau PET positivity will facilitate its use for clinical practice and research. Here we conducted an analysis of 42 cohorts worldwide (N = 12,048), including 7,394 cognitively unimpaired (CU) participants, 2,177 participants with mild cognitive impairment (MCI) and 2,477 participants with dementia. We found that from age 60 years to 80 years, tau PET positivity in a temporal composite region increased from 1.1% to 4.4% among CU amyloid-β (Aβ)-negative participants and from 17.4% to 22.2% among CU Aβ-positive participants. Across the same age span, tau PET positivity decreased from 68.0% to 52.9% in participants with MCI and from 91.5% to 74.6% in participants with dementia. Age, Aβ status, APOE ε4 carriership and female sex were all associated with a higher prevalence of tau PET positivity across groups. APOE ε4 carriership in CU individuals lowered the age at onset of both Aβ positivity and tau positivity by decades. Finally, we replicated these associations in an independent autopsy dataset (N = 5,072 from 3 cohorts).
© 2025. The Author(s).
Conflict of interest statement
Competing interests: R.O. received research support from Avid Radiopharmaceuticals, Janssen Research & Development, Roche, Quanterix and Optina Diagnostics. He has given lectures in symposia sponsored by GE Healthcare and serves on advisory boards and/or steering committees for Asceneuron, Biogen and Bristol Myers Squibb. All of the above is paid to his institutions. E.v.d.G. received research support from NWO, ZonMw, Hersenstichting, Alzheimer Nederland, Health-Holland and KWF. J.T. is funded by the Colin J. Adair Charitable Foundation fellowship. Funding for the TRIAD cohort comes from the Weston Brain Institute, Canadian Institutes of Health Research (CIHR) (grant nos. MOP-11-51-31; RFN 152985, 159815 and 162303), Canadian Consortium of Neurodegeneration and Aging (CCNA; grant no. MOP-11-51-31-team 1), the Alzheimer’s Association (grant nos. NIRG-12-92090 and NIRP-12-259245), Brain Canada Foundation (CFI, project no. 34874. grant no. 33397), the Fonds de Recherche du Québec—Santé (FRQS; Chercheur Boursier, grant no. 2020-VICO-279314) and the Colin J. Adair Charitable Foundation. A.d.B. received research funding from Alzheimer Association, Alzheimer Nederland, Stichting Dioraphte, Health Holland, Weston Brain Institute and Selfridges Group Foundation. A.J.S. receives support from multiple National Institutes of Health (NIH) grants. He has also received support from Avid Radiopharmaceuticals, a subsidiary of Eli Lilly (in kind contribution of PET-tracer precursor) and participated in scientific advisory boards (Bayer Oncology, Eisai, Novo Nordisk and Siemens Medical Solutions USA, Inc.) and an Observational Study Monitoring Board (MESA, NIH, National Heart, Lung, and Blood Institute), as well as external advisory committees for multiple National Institute on Aging (NIA) grants. He also serves as Editor-in-Chief of Brain Imaging and Behavior, a Springer Nature Journal. J.B.R. is supported by the Medical Research Council (MRC, grant nos. MC_UU_00030/14 and MR/T033371/1) and National Institute for Health and Care Research (NIHR) Cambridge Biomedical Research Centre (grant no. NIHR203312), the PSP Association and the Cambridge Centre for Parkinson-plus. M.M. is supported by Race Against Dementia Alzheimer’s Research UK (grant no. ARUK-RADF2021A-010), NIHR Cambridge Biomedical Research Centre (grant no. NIHR203312) and the UK Dementia Research Institute through UK DRI Ltd, principally funded by the MRC. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care. J.M.S. acknowledges the support of the NIHR University College London Hospitals Biomedical Research Centre, Wolfson Foundation, Alzheimer’s Research UK, Brain Research UK, Weston Brain Institute, MRC, British Heart Foundation, UK Dementia Research Institute and Alzheimer’s Association. J.M.S. received research funding and PET tracer from AVID Radiopharmaceuticals (a wholly owned subsidiary of Eli Lilly) and Alliance Medical, has consulted for Roche, Eli Lilly, Biogen, AVID, Merck and GE and is Chief Medical Officer for Alzheimer’s Research UK. V.G. was funded from the Swiss National Science Foundation (project nos. 320030_169876 and 320030_185028), VELUX Foundation, Schmidheiny Foundation and Fondation Privée of the University Hospitals of Geneva. Research programs of W.M.v.d.F. have been funded by ZonMW, NWO, EU-JPND, EU-IHI, Alzheimer Nederland, Hersenstichting CardioVascular Onderzoek Nederland, Health-Holland, Topsector Life Sciences & Health, stichting Dioraphte, Gieskes-Strijbis fonds, stichting Equilibrio, Edwin Bouw fonds, Noaber foundation, Pieter Houbolt Fonds, Pasman stichting, stichting Alzheimer & Neuropsychiatrie Foundation, Philips, Biogen MA Inc, Novartis-NL, Life-MI, AVID, Roche BV, Fujifilm, Eisai and Combinostics. W.M.v.d.F. holds the Pasman chair and is recipient of ABOARD, which is a public–private partnership receiving funding from ZonMW (grant no. 73305095007) and Health-Holland, Topsector Life Sciences & Health (PPP-allowance; grant no. LSHM20106). She is a recipient of TAP-dementia ( www.tap-dementia.nl ), receiving funding from ZonMw (grant no. 10510032120003) in the context of Onderzoeksprogramma Dementie, part of the Dutch National Dementia Strategy. TAP-dementia receives co-financing from Avid Radiopharmaceuticals, Roche Diagnostics and Amprion. Gieskes-Strijbis Fonds also contributes to TAP-dementia. W.M.v.d.F. has been an invited speaker at Biogen MA Inc, Danone, Eisai, WebMD Neurology (Medscape), Novo Nordisk, Springer Healthcare and European Brain Council. She is a consultant to Oxford Health Policy Forum CIC, Roche, Biogen MA Inc. and Eisai, and participated in advisory boards of Biogen MA Inc., Roche, and Eli Lilly. W.M.v.d.F. is a member of the steering committee of EVOKE/EVOKE+ (Novo Nordisk). All funding is paid to her institution. She is member of the steering committee of PAVE and Think Brain Health. S.K. was financed by grants from the Swedish state under the agreement between the Swedish Government and the county councils, the ALF agreement (grant nos. ALFGBG-965923, ALFGBG-81392 and ALFGBG-771071). The Alzheimerfonden (grant nos. AF-842471, AF-737641, AF-929959 and AF-939825). The Swedish Research Council (grant nos. 2019-02075 and 2019-02075_15) and Stiftelsen Psykiatriska Forskningsfonden. S.P. has acquired research support (for the institution) from ki elements/ADDF and Avid. In the past 2 years, he has received consultancy or speaker fees from Bioartic, Biogen, Esai, Lilly and Roche. M.M. provides consultancy unrelated to the current work to Astex Pharmaceuticals. J.T. has served as a consultant for the Neurotorium educational platform and for Alzheon. P.R.-N. has served at scientific advisory boards and/or as a consultant for Roche, Novo Nordisk, Eisai and Cerveau Radiopharmaceuticals. C.C.R. has received research grants from National Health and Medical Research Council (NHMRC), Enigma Australia, Biogen, Eisai and Abbvie. He is on the scientific advisory board for Enigma/Mellieur Technologies and has consulted for Prothena, Eisai, Roche and Biogen Australia. S.C.J. has served in the past 2 years on advisory boards for Enigma Biomedical and ALZPath. K.V.L. has received research grants through KU Leuven from Biogen, BMS, Cerevel, CHDI, Janssen Pharmaceuticals, Lantheus/Cerveau, Lundbeck and Rapport. He is a member of the scientific advisory board for Enigma/Mellieur Technologies. V.G. received research support and speaker fees through her institution from GE Healthcare, Siemens Healthineers, Novo Nordisk. Janssen and Novartis. S.K. has served at scientific advisory boards, speaker and/or consultant for Roche, Eli Lilly, Geras Solutions, Optoceutics, Biogen and Bioarctic. S.S., M.P. and I.K. are employees and minor shareholders of Eli Lilly and Co. A.D. received research support from Siemens Healthineers, Life Molecular Imaging, GE Healthcare, AVID Radiopharmaceuticals, Sofie, Eisai, Novartis/AAA and Ariceum Therapeutics. He received speaker or honorary fees and/or contributed to advisory boards for Siemens Healthineers, Sanofi, GE Healthcare, Biogen, Novo Nordisk, Invicro, Novartis/AAA, Bayer Vital, Lilly, Peer View Institute for Medical Education and the International Atomic Energy Agency. He holds stock from Siemens Healthineers, Lantheus Holding, Structured therapeutics, Lilly and a patent for 18F-JK-PSMA-7 (PSMA PET imaging tracer; patent no. EP3765097A1; date of patent: 20 January 2021). He has received national and international grants including DFG grants (nos. SFB 1451 C04 and DR 445/9-1) and serves as Associate Editor of the Journal of Nuclear Medicine. L.A. received personal compensation for serving as a consultant for Biogen, Two Labs, Florida Department of Health, Genetech, NIH Biobank, Eli Lilly, GE Healthcare, Eisai and Roche Diagnostics and for serving on a Data Safety and Monitoring Board for IQVIA. L.A. receives research support from the National Institute on Aging, the Alzheimer’s Association, Roche Diagnostics, AVID radiopharmaceuticals, Life Molecular Imaging and Eli Lilly. G.B.F. received funding through the Private Foundation of Geneva University Hospitals from: APRA (Association Suisse pour la Recherche sur la Maladie d’Alzheimer), Geneva; Fondation Segré, Geneva; Ivan Pictet, Geneva; Race Against Dementia Foundation, London, UK; Fondation Child Care, Geneva; Fondation Edmond J. Safra, Geneva; Fondation Minkoff, Geneva; Fondazione Agusta, Lugano; McCall Macbain Foundation, Canada; Nicole et René Keller, Geneva; Fondation AETAS, Geneva. He has also received funding through the University of Geneva or Geneva University Hospitals: for IISSs from ROCHE Pharmaceuticals OM Pharma EISAI Pharmaceuticals Biogen Pharmaceuticals and Novo Nordisk; and funding for competitive research projects from: H2020, Innovative Medicines Initiative (IMI), IMI2, Swiss National Science Foundation and VELUX Foundation; consulting fees from: Biogen, Diadem and Roche; and payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from: Biogen, Roche, Novo Nordisk and GE HealthCare. W.J.J. serves on data monitoring committees for Lilly, holds equity in Optoceutics and Molecular Medicine, receives research support from Biogen and grants from ZonMW, Alzheimer Nederland, St. Rinsum-Ponsen. A.M.B. has received payment for consulting or participation in advisory boards from Cognition Therapeutics, Cognito Therapeutics and CogState. He is a section editor for Alzheimer’s & Dementia. J.O.’B. has acted as a consultant for TauRx, Novo Nordisk, Biogen, Roche, Lilly, GE Healthcare and Okwin and received grants or academic support from Avid/Lilly, Merck and Alliance Medical. J.A.L. received royalties from Spring for the book Diabetes in the Brain, a stipend from Wolters Kluwer as editor of the journal Alzheimer’s Disease and Associated Disorders, and donated drug and placebo for an NIH-funded clinical trial from EMD Serono. He was a consultant to Merck KGaA in 2022 and to Novo Nordisk in 2024 and 2025. J.D.-G. received research support from GE HealthCare, Roche Diagnostics, Hoffmann—La Roche and Life—MI; participated in symposia sponsored by Biogen, Philips Nederlands, Life-MI and Esteve; acted as a consultant for Roche Diagnostics; and served in the Molecular Neuroimaging Advisory Board of Prothena Biosciences. J.D.-G. is founder, co-owner and member of the Board of Directors of Betascreen SL and is currently a full-time employee of AstraZeneca. W.C.K. has served as a consultant for Cerveau Technologies, Inc. O.H. is an employee of Eli Lilly and Lund University, and he has previously acquired research support (for Lund University) from AVID Radiopharmaceuticals, Biogen, C2N Diagnostics, Eli Lilly, Eisai, Fujirebio, GE Healthcare and Roche. In the past 2 years, he received consultancy or speaker fees from Alzpath, BioArctic, Biogen, Bristol Meyer Squibb, Eisai, Eli Lilly, Fujirebio, Merck, Novartis, Novo Nordisk, Roche, Sanofi and Siemens. Work at Lund University was supported by the ERC (grant no. ADG-101096455), Alzheimer’s Association (grant nos. ZEN24-1069572 and SG-23-1061717), GHR Foundation, Swedish Research Council (grant no. 2022-00775), ERA PerMed (grant no. ERAPERMED2021-184), Knut and Alice Wallenberg foundation (grant no. 2022-0231), Strategic Research Area MultiPark (Multidisciplinary Research in Parkinson’s disease) at Lund University, Swedish Alzheimer Foundation (grant no. AF-980907), Swedish Brain Foundation (grant no. FO2021-0293), Parkinson Foundation of Sweden (grant no. 1412/22), Cure Alzheimer’s fund, Rönström Family Foundation, Konung Gustaf V:s och Drottning Victorias Frimurarestiftelse, Skåne University Hospital Foundation (grant no. 2020-O000028), Regionalt Forskningsstöd (grant no. 2022-1259) and Swedish Federal Government under the ALF agreement (grant no. 2022-Projekt0080). The precursor of [18F]flortaucipir was provided by AVID radiopharmaceuticals and the precursor of [18F]RO948 by Roche. The precursor of [18F]flutemetamol was sponsored by GE Healthcare. The MCSA is supported by the National Institute on Aging (grant no. U01 AG006786), GHR and the Alzheimer’s Association. G.S. received funding from the European Union’s Horizon 2020 Research and Innovation Program under Marie Sklodowska-Curie action (grant no. 101061836), an Alzheimer’s Association Research Fellowship (no. AARF-22-972612), the Alzheimerfonden (grant no. AF-980942), Greta och Johan Kocks research grants and travel grants from the Strategic Research Area MultiPark (Multidisciplinary Research in Parkinson’s Disease) at Lund University. The data contributed from Columbia University Irving Medical Center were supported by grant funding from the NIA (grant nos. K23AG052633, R01AG063888, P30AG066462, R01AG055299, RF1AG051556, R01AG050440, R01AG055299, K24AG045334 and R00AG065506). Funding for data from Stanford University was supported by NIA (grant nos. P30AG066515 and R01AG074339 to E.C.M. and K99AG071837 to C.B.Y.) and National Institute of Neurological Disorders and Stroke (grant no. R01NS115114). The data contributed from the Shatau7-IMATAU study (Paris) were supported by French Ministry of Health (grant no. PHRC-2013-0919), CEA, Fondation pour la recherche sur Alzheimer, Institut de Recherches Internationales Servier, France-Alzheimer. The MCSA is supported by the NIA (grant no. U01 AG006786), GHR and the Alzheimer’s Association. The data contributed from the Wisconsin Registry for Alzheimer’s Prevention were supported by grant funding from the NIA to the University of Wisconsin (grant nos. R01 AG021155 and R01 AG027161 to S.C.J.). Funding for data from Washington University was supported by the NIA (grant nos. R01AG070941 to S.E.S., P30AG066444, P01AG003991 and P01AG026276 to J.C.M.). Blood plasma measurements were supported by grant nos. RF1AG061900 (to R.J.B), R56AG061900 (to R.J.B.) and the Tracy Family SILQ Center (to R.J.B.). The data contributed from the PREVENT-AD were supported by public–private partnership funds provided by McGill University, the Fonds de Recherche du Québec—Santé (FRQ-S), an unrestricted research grant from Pfizer Canada, the Levesque Foundation, the Douglas Hospital Research Centre and Foundation, the Government of Canada, the Canada Fund for Innovation, the Canadian Institutes of Health Research, the Alzheimer Society of Canada, the US NIH, the Alzheimer Association and Brain Canada Foundation. Data collection and dissemination of the data presented in this manuscript were supported by the LEADS Consortium (grant nos. R56/U01 AG057195, funded by the NIA, as well as grant no. U24AG021886, Alzheimer’s Association, LEADS GENETICS‐19‐639372, LDRFP-21-818464, Alzheimer’s LDRFP-21-824473 and LDRFP-21-828356). NACC is funded by the NIA (grant no. U24 AG072122). NACC data are contributed by the following NIA-funded ADRCs: P30 AG010133, P30 AG062422, P30 AG066462, P30AG066507, P30 AG062421, P30 AG066506, P30AG072977, P30 AG066444, P30 AG066515, P30 AG062677, P30 AG072980, P30 AG072979 and P30 AG066511. The manuscript has been reviewed by the LEADS Publication Committee for scientific content. We acknowledge the invaluable contributions of the participants in LEADS as well as the assistance of the investigators and support staff at each of the participating sites. The ALFA study receives funding from ‘la Caixa’ Foundation (ID 100010434), under agreement no. LCF/PR/GN17/50300004, the Alzheimer’s Association and an international anonymous charity foundation through the TriBEKa Imaging Platform project (TriBEKa-17-519007). Additional support has been received from the Universities and Research Secretariat, Ministry of Business and Knowledge of the Catalan Government under grant no. 2021 SGR 00913. Data were obtained from Australian Imaging Biomarkers and Lifestyle (AIBL) flagship study of aging and the Australian Dementia Network funded by the NHMRC of Australia (grant nos. APP1132604, APP1140853 and APP1152623), a grant from Enigma Australia and support from the Commonwealth Scientific and Industrial Research Organization (CSIRO). The Banner Sun Health Research Institute Brain and Body Donation Program has been supported by the National Institute of Neurological Disorders and Stroke (grant no. U24 NS072026, National Brain and Tissue Resource for Parkinson’s Disease and Related Disorders), the NIA (grant nos. P30AG019610 and P30AG072980, Arizona Alzheimer’s Disease Center), the Arizona Department of Health Services (contract no. 211002, Arizona Alzheimer’s Research Center), the Arizona Biomedical Research Commission (contract nos. 4001, 0011, 05-901 and 1001 to the Arizona Parkinson’s Disease Consortium) and the Michael J. Fox Foundation for Parkinson’s Research. The NACC database is funded by the NIA (grant no. U01 AG016976). Data collection and sharing for this project were funded by the ADNI (NIH, grant no. U01 AG024904) and DOD ADNI (Department of Defense award no. W81XWH-12-2-0012). ADNI is funded by the NIA, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Co.; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research provides funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the NIH ( www.fnih.org ). The grantee organization is the Northern California Institute for Research and Education and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California. ROSMAP is supported by grant nos. P30AG10161, P30AG72975, R01AG15819, R01AG17917, U01AG46152 and U01AG61356. ROSMAP resources can be requested at https://www.radc.rush.edu and www.synpase.org . The other authors declare no competing interests.
Figures


References
-
- Gustavsson, A. et al. Global estimates on the number of persons across the Alzheimer’s disease continuum. Alzheimers Dement.19, 658–670 (2023). - PubMed
-
- Klunk, W. E. et al. Imaging brain amyloid in Alzheimer’s disease with Pittsburgh Compound-B. Ann. Neurol.55, 306–319 (2004). - PubMed
-
- Chien, D. T. et al. Early clinical PET imaging results with the novel PHF-tau radioligand [F-18]-T807. J. Alzheimers Dis.34, 457–468 (2013). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
