

The diagnostic accuracy of the ESC 0/1-hour algorithm in non-ST-segment elevation myocardial infarction in a crowded emergency department: a real-world experience from a single-center in Türkiye
- PMID: 40670967
- PMCID: PMC12269136
- DOI: 10.1186/s12873-025-01289-7
The diagnostic accuracy of the ESC 0/1-hour algorithm in non-ST-segment elevation myocardial infarction in a crowded emergency department: a real-world experience from a single-center in Türkiye
Abstract
Background: The rapid and accurate diagnosis of non-ST-segment elevation myocardial infarction (NSTEMI) is critical to improving patient outcomes and reducing emergency department (ED) overcrowding. The European Society of Cardiology (ESC) 0/1-hour algorithm, utilizing high-sensitivity cardiac troponin T (hs-cTnT) levels, has demonstrated high diagnostic performance internationally. This study aimed to evaluate its diagnostic accuracy in a high-volume ED setting in Türkiye.
Methods: This single-center retrospective cohort study was conducted at Marmara University Pendik Training and Research Hospital, Türkiye, from September 1 to December 31, 2022. Adults presenting with acute chest discomfort and undergoing hs-cTnT testing per the ESC 0/1-hour algorithm were included. Patients with ST-segment elevation, missing data, pregnancy, or those discharged against medical advice were excluded. The primary outcome was NSTEMI diagnosis; the secondary outcome was major adverse cardiac events (MACE) within 30 days.
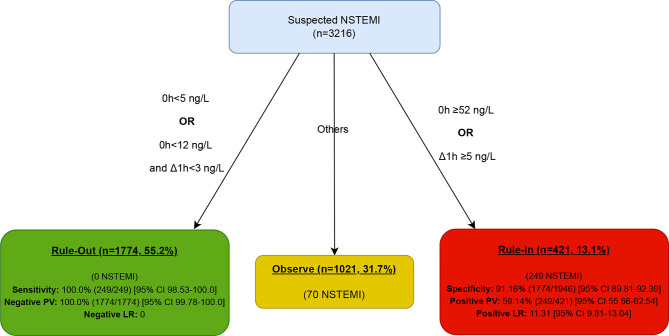
Results: Of 3,529 eligible patients, 3,216 were included. The mean age of the patients was 53.9 ± 16.4 years, and 58.3% were male. NSTEMI was diagnosed in 319 patients (9.9%). According to the ESC algorithm, 54.4% of patients were classified as "rule-out," 31.3% as "observe," and 12.3% as "rule-in." The sensitivity and negative predictive value (NPV) for NSTEMI in the "rule-out" group were both 100%. In the "rule-in" group, the specificity was 91.16%, and the positive predictive value (PPV) was 59.14%. MACE occurred in 13.6% (436 patients) within 30 days: 0.7% in the "rule-out" group, 13.9% in the "observe" group, and 67.0% in the "rule-in" group.
Conclusions: The ESC 0/1-hour algorithm is highly effective for ruling out NSTEMI in Türkiye, demonstrating excellent sensitivity and NPV. While it facilitates early discharge of low-risk patients, enhancements are needed for risk stratification in intermediate-risk groups. Its implementation could optimize ED resource utilization and improve clinical outcomes.
Clinical trial number: Not applicable.
Keywords: Acute coronary syndrome; Diagnostic accuracy; ESC algorithms; High sensitivity troponin; Myocardial infarction.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Marmara University Clinical Research Ethics Committee approved the study protocol (protocol number: 09.2023.960), and the study was conducted in accordance with the Declaration of Helsinki. Since the study was conducted retrospectively, informed consent was not obtained from the patients. For patients contacted via phone, verbal informed consent was first obtained, and subsequently, outcome data were collected either through direct communication with the patient or by accessing their electronic health records. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests.
Figures

References
-
- Menekşe TS, et al. C-reactive protein to albumin ratio may predict in-hospital mortality in non-ST elevation myocardial infarction. Biomark Med. 2024;18(3):103–13. - PubMed
-
- Gulati M, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: Executive summary: A report of the American college of Cardiology/American heart association joint committee on clinical practice guidelines. Circulation. 2021;144(22):e368–454. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
