

Multiple evanescent white dot syndrome associated with focal scleral nodule: a case report and literature review
- PMID: 40671005
- PMCID: PMC12265223
- DOI: 10.1186/s12886-025-04231-4
Multiple evanescent white dot syndrome associated with focal scleral nodule: a case report and literature review
Abstract
Background: Multiple evanescent white dot syndrome (MEWDS) is a rare transient inflammatory retinopathy characterized by discrete white dots disseminated on the fundus. Focal scleral nodule (FSN) typically presents as a stable, solitary, yellow-white, subretinal lesion arising from the sclera. This article reports a rare case of MEWDS associated with FSN in a young female.
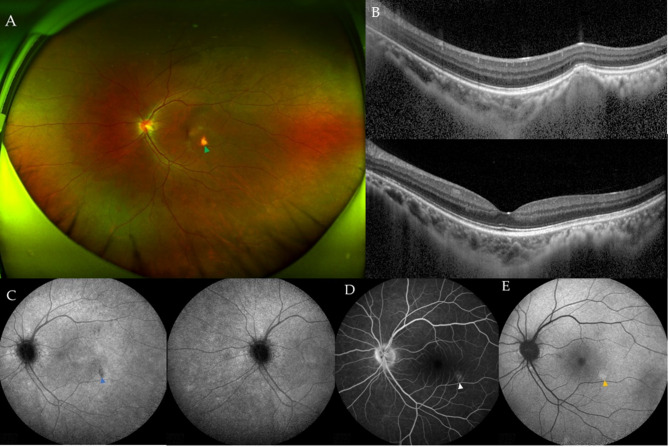
Case presentation: A 34-year-old female presented with a complaint of gradually enlarging paracentral scotomas in the left eye for 8 days. At presentation, best-corrected visual acuity (BCVA) was 20/25 in the left eye. Fundus examination of the left eye revealed optic disc edema and an orange-yellow irregular lesion on the infratemporal side of the fovea. The multimodal imaging (MMI) findings revealed a rather typical MEWDS-like reaction and a subretinal lesion located at the sclera. After thorough consideration, the patient was diagnosed with MEWDS associated with FSN. Corticosteroid therapy was then administered to the patient. After 11 weeks, her BCVA recovered to 20/20 in the left eye, and the visual field defect had improved. Additionally, the MEWDS-like reaction had significantly recovered. The FSN remained stable during the 18-month follow-up.
Conclusions: This is the first reported case of MEWDS associated with FSN, expanding the understanding of both conditions.
Keywords: Case report; Focal scleral nodule; MEWDS-like reaction; Multiple evanescent white Dot syndrome; Review; Secondary MEWDS.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was performed in accordance with the tenets of the Declaration of Helsinki. Consent to participate was not applicable due to the retrospective design of this study. Consent for publication: Written informed consent was obtained from the patient for the publication of this report and the accompanying images. Competing interests: The authors declare no competing interests.
Figures




References
-
- Jampol LM, Sieving PA, Pugh D, Fishman GA, Gilbert H. Multiple evanescent white dot syndrome. I Clinical findings Arch Ophthalmol. 1984;102(5):671–4. - PubMed
-
- Serrar Y, Cahuzac A, Gascon P, Langlois-Jacques C, Mauget-Faÿsse M, Wolff B, Sève P, Kodjikian L, Mathis T. Comparison of primary and secondary forms of multiple evanescent white dot syndrome. Retina. 2022;42(12):2368–78. - PubMed
-
- Meng Y, Zhang Q, Li L, Yi Z, Xu Y, Su Y, Liang C, Xiao D, Zhang L, Chen C. Primary multiple evanescent white dot syndrome and multiple evanescent white dot syndrome secondary to multifocal choroiditis/punctate inner choroidopathy: a comparative study. Retina. 2023;43(7):1122–31. - PubMed
-
- Pichi F, Srvivastava SK, Chexal S, Lembo A, Lima LH, Neri P, Saitta A, Chhablani J, Albini TA, Nucci P, et al. En face optical coherence tomography and optical coherence tomography angiography of multiple evanescent white dot syndrome: new insights into pathogenesis. Retina. 2016;36 Suppl 1:S178-s188. - PubMed
-
- Marsiglia M, Gallego-Pinazo R, Cunha de Souza E, Munk MR, Yu S, Mrejen S, Cunningham ET, Jr., Lujan BJ, Goldberg NR, Albini TA, et al. Expanded clinical spectrum of multiple evanescent white dot syndrome with multimodal imaging. Retina. 2016, 36(1):64–74. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
