

The initial stage of alveolar echinococcosis is a diagnostic challenge: a case report
- PMID: 40671141
- PMCID: PMC12265298
- DOI: 10.1186/s13256-025-05298-9
The initial stage of alveolar echinococcosis is a diagnostic challenge: a case report
Abstract
Background: Alveolar echinococcosis is a rare, potentially fatal parasitosis with the main manifestation site in the liver. Diagnosis already in the initial stage of the disease is important to prevent further exacerbation and possible secondary complications by early targeted therapy. Identifying alveolar echinococcosis lesions on imaging can be difficult, and making the diagnosis can be an interdisciplinary challenge, even in a specialized center.
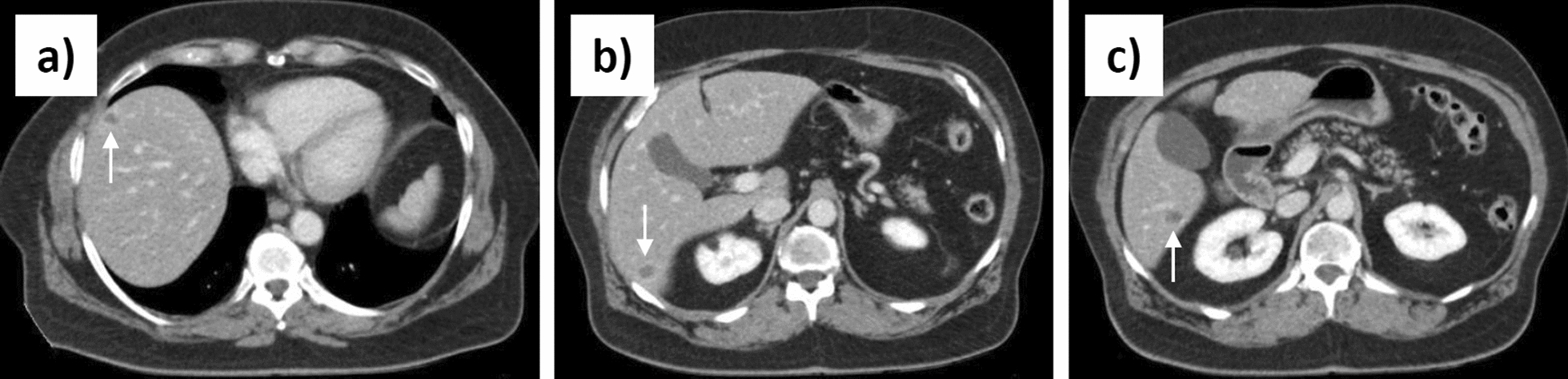
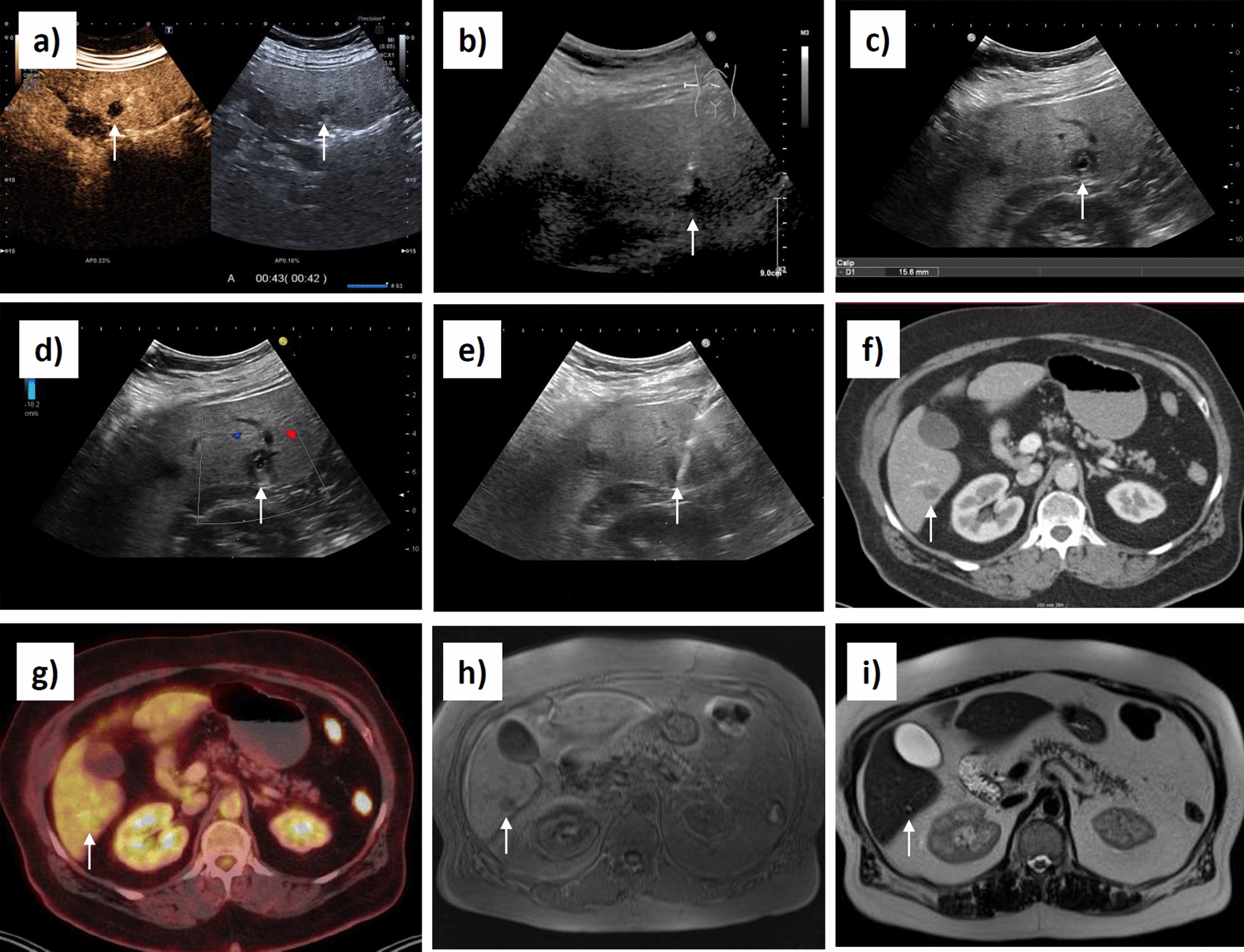
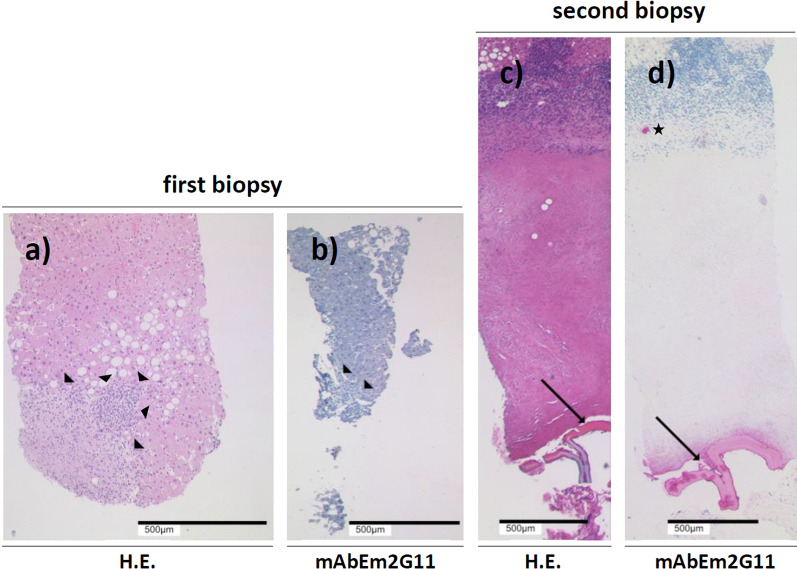
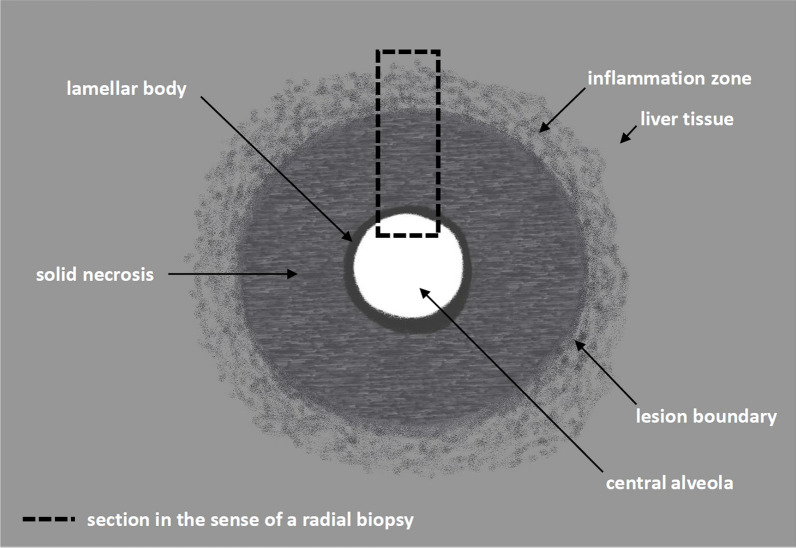
Case presentation: In a clinically symptom-free 65-year-old white female patient with type 2 diabetes mellitus, an abdominal ultrasonography performed by a colleague in private practice revealed three small hepatic nodules as incidental findings. Further workup focused primarily on the differential diagnosis of hepatic metastatic malignancy. Therefore, a sonographically guided biopsy of the liver lesions was performed under inpatient conditions. During the control sonography routinely performed after the biopsy to exclude postinterventional hemorrhage, an examiner previously uninvolved in the case noticed the typical sonomorphology of initial alveolar echinococcosis lesions in view of the biopsied nodules. The specimens that had been collected peripherally from the target lesion under the primary assumption of metastases histopathologically showed no signs of malignancy and no other landmark findings. Follow-up staining of the biopsies with regard to the recently suspected diagnosis of alveolar echinococcosis, however, remained without a target result as well. Due to the typical sonomorphology, a further biopsy was performed. During rebiopsy, the target lesion was deliberately biopsied centrally to hit the presumed annular lamellar body localized there in alveolar echinococcosis. On the basis of the samples of the second biopsy, the diagnosis of alveolar echinococcosis in the initial stage could be confirmed histopathologically, and the patient was transferred to adequate therapy.
Conclusion: One of the most important differential diagnoses of hepatic alveolar echinococcosis in the initial stage is liver metastases. Knowledge of the typical sonomorphology is essential to avoid misdiagnosis. In addition, proper localization of specimen collection within an alveolar echinococcosis initial lesion is critical to enable histopathologic diagnosis. Imaging and pathology are directly complementary, and imaging can point the way to the correct histopathologic diagnosis on the basis of lesion morphology. For this, knowledge of the specifics of alveolar echinococcosis in imaging and histomorphology is necessary to integratively combine the findings.
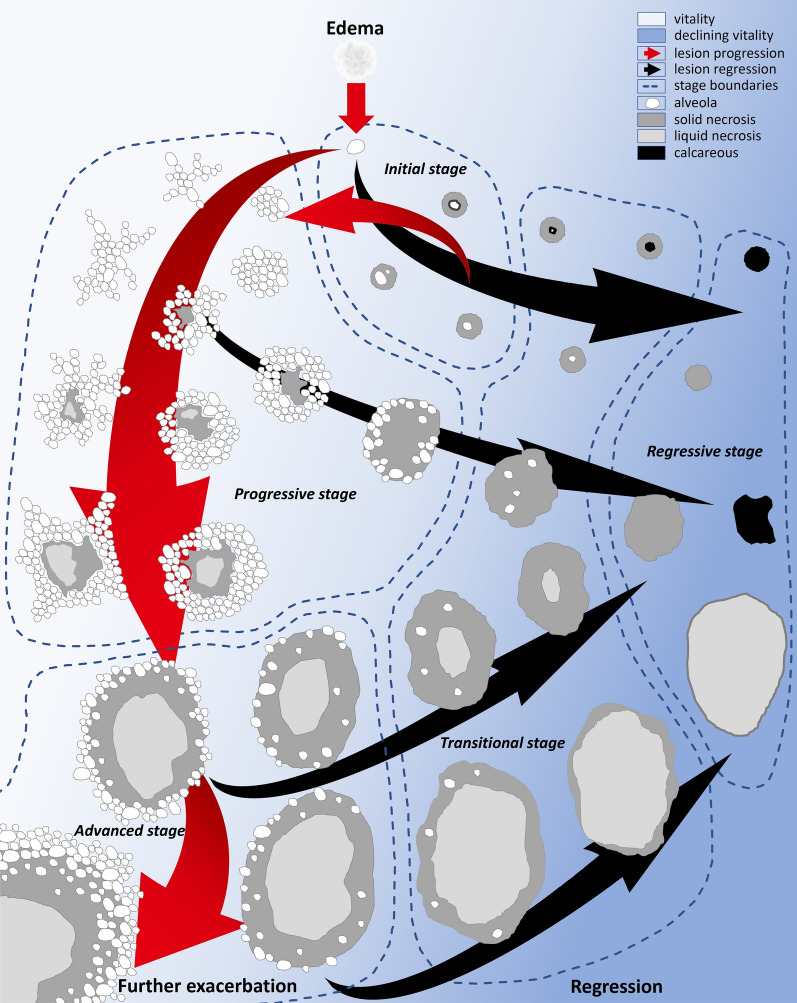
Keywords: Alveolar echinococcosis; Evolution model; Histopathology; Imaging diagnostics; Initial stage.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal. Competing interests: The authors declare that they have no competing interests.
Figures
Similar articles
-
Contrast-enhanced ultrasound using SonoVue® (sulphur hexafluoride microbubbles) compared with contrast-enhanced computed tomography and contrast-enhanced magnetic resonance imaging for the characterisation of focal liver lesions and detection of liver metastases: a systematic review and cost-effectiveness analysis.Health Technol Assess. 2013 Apr;17(16):1-243. doi: 10.3310/hta17160. Health Technol Assess. 2013. PMID: 23611316 Free PMC article.
-
Intraoperative frozen section analysis for the diagnosis of early stage ovarian cancer in suspicious pelvic masses.Cochrane Database Syst Rev. 2016 Mar 1;3(3):CD010360. doi: 10.1002/14651858.CD010360.pub2. Cochrane Database Syst Rev. 2016. PMID: 26930463 Free PMC article.
-
Can a Liquid Biopsy Detect Circulating Tumor DNA With Low-passage Whole-genome Sequencing in Patients With a Sarcoma? A Pilot Evaluation.Clin Orthop Relat Res. 2025 Jan 1;483(1):39-48. doi: 10.1097/CORR.0000000000003161. Epub 2024 Jun 21. Clin Orthop Relat Res. 2025. PMID: 38905450
-
Magnetic resonance imaging for the diagnosis of hepatocellular carcinoma in adults with chronic liver disease.Cochrane Database Syst Rev. 2022 May 6;5(5):CD014798. doi: 10.1002/14651858.CD014798.pub2. Cochrane Database Syst Rev. 2022. PMID: 35521901 Free PMC article.
-
123I-MIBG scintigraphy and 18F-FDG-PET imaging for diagnosing neuroblastoma.Cochrane Database Syst Rev. 2015 Sep 29;2015(9):CD009263. doi: 10.1002/14651858.CD009263.pub2. Cochrane Database Syst Rev. 2015. PMID: 26417712 Free PMC article.
References
-
- Moro P, Schantz PM. Echinococcosis: a review. Int J Infect Dis. 2009;13(2):125–33. 10.1016/j.ijid.2008.03.037. - PubMed
-
- Ammann RW, Eckert J. Cestodes. Echinococcus Gastroenterol Clin North Am. 1996;25(3):655–89. 10.1016/s0889-8553(05)70268-5. - PubMed
-
- Bresson-Hadni S, Spahr L, Chappuis F. Hepatic alveolar echinococcosis. Semin Liver Dis. 2021;41(3):393–408. 10.1055/s-0041-1730925. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
