

Restraint for nasogastric tube feeding in young people with anorexia nervosa or atypical anorexia nervosa: a retrospective audit
- PMID: 40671143
- PMCID: PMC12269248
- DOI: 10.1186/s40337-025-01342-7
Restraint for nasogastric tube feeding in young people with anorexia nervosa or atypical anorexia nervosa: a retrospective audit
Abstract
Background: Medically unstable young people with anorexia nervosa or atypical anorexia nervosa, are admitted to the adolescent medical ward at the reporting institution for nutritional rehabilitation. If meals are refused a nasogastric tube may be needed. At times restraint is used to ensure the required feeds are administered. This is an ethically complex and distressing dilemma for all involved and can result in long-term trauma for young people. The aim of this project was to establish a profile of young people with anorexia nervosa or atypical anorexia nervosa who require restraint for nasogastric tube insertion and/or feeding in the acute care paediatric setting and to understand the extent of restraint events occurring.
Method: We undertook a retrospective audit of inpatients admitted to the adolescent medical ward at a quaternary pediatric hospital in Melbourne, Australia, between 2021 and 2023, for the treatment of anorexia nervosa or atypical anorexia nervosa. Data points were agreed by multidisciplinary stakeholders and were collected from the institution's electronic medical record. Data were analysed using descriptive statistics.
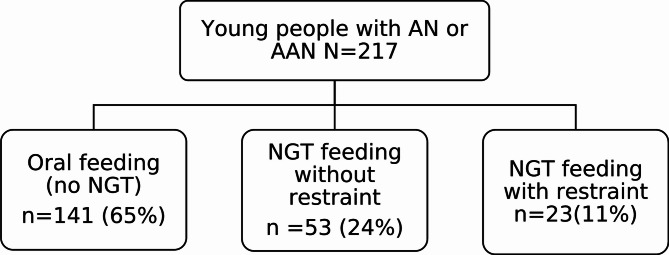
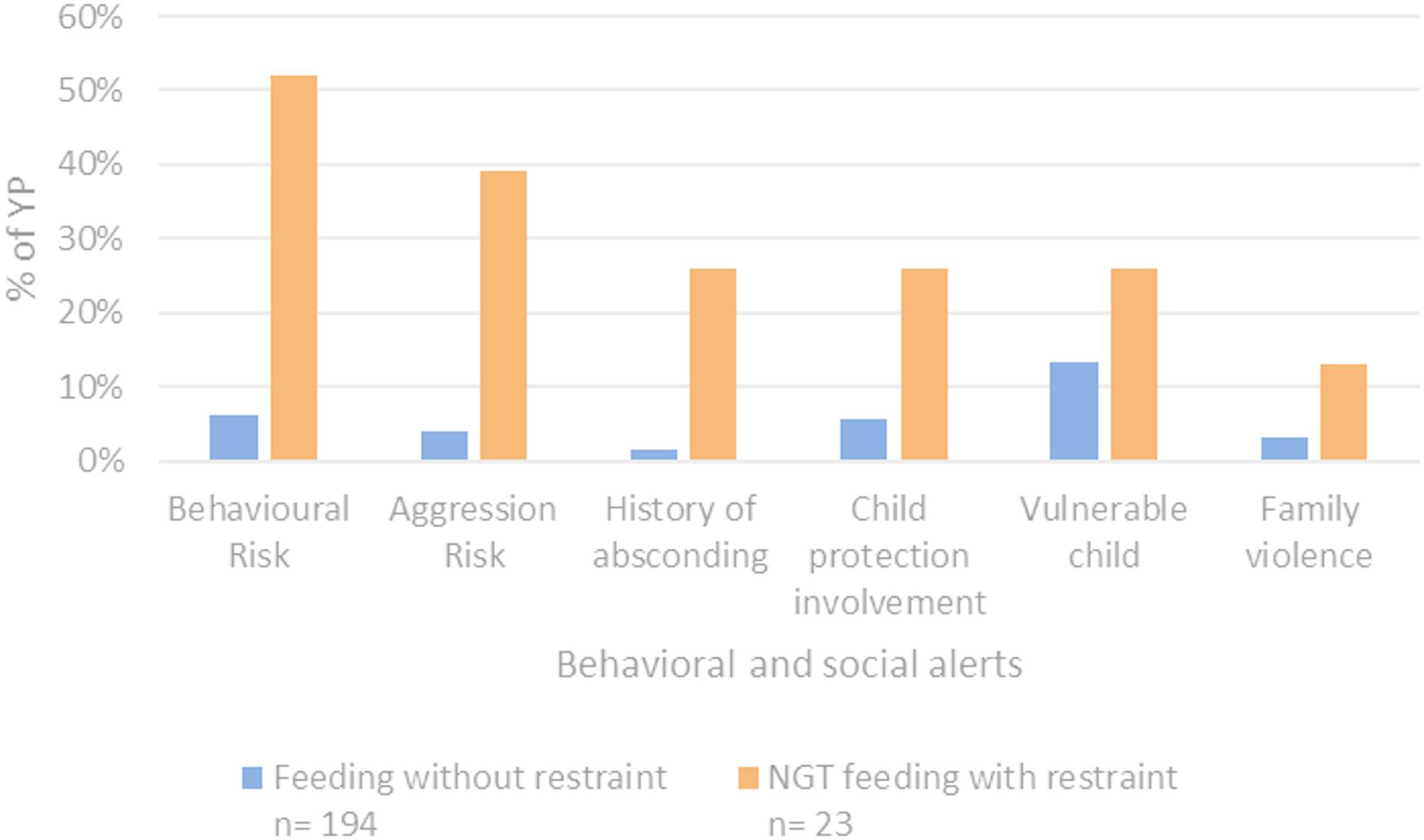
Results: Of the 217 young people admitted, 23 (11%) had documented physical restraint for nasogastric tube feeding. Mental health comorbidities, neurodivergence, and social or behavioural complexity were higher in the young people who required feeding restraint as compared to those that did not. Of note, 15 (65%) of young people who were restrained for feeds had a diagnosis of autism, or a clinical note in their medical record indicating possible autism.
Conclusions: Young people in our institution admitted to the adolescent medical ward with anorexia nervosa or atypical anorexia nervosa who are restrained for feeding have a more complex clinical, social and behavioural profile than those who do not require restraint. Care and treatment tailored to the individual, sensitive to neurodivergence, encourages clinicians to consider the young person they are treating to reduce or prevent restraint and to inform a restraint approach that mitigates iatrogenic harm.
Keywords: Anorexia nervosa; Atypical anorexia nervosa; Autism; Nasogastric tube; Paediatric; Physical restraint; Restraint.
Plain language summary
Young people who are inpatients on a medical ward when critically unwell with anorexia may require a nasogastric tube for nutrition when oral intake is inadequate. If the young person requires a nasogastric tube but refuses, they may be restrained for this urgent medical treatment. Those who are more likely to be restrained for nasogastric tube feeding might be identified through their more complex social, behavioural and clinical profiles. Importantly, there is an overrepresentation of those with a diagnosis of autism or clinical suspicion of autism, experiencing restraint for feeding via a nasogastric tube. For these young people, individualised care, sensitive to neurodivergence for an admission for medical stabilisation, may reduce the need for restraint to feed and minimise potential harm due to medical treatment.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by The Royal Children’s Hospital Research and Ethics Committee’s quality assurance pathway, number VIC104256. This HREC is organised and operates in line with the - National Health and Medical Research Council’s (NHMRC) National Statement on Ethical Conduct in Human Research (2007), and all subsequent updates; Note for Guidance on Good Clinical Practice (CPMP/ICH/135/95); Health Privacy Principles described in the Health Records Act 2001 (Vic) and Section 95 A of the Privacy Act 1988, and subsequent guidelines. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Sexual Harassment and Prevention Training.2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 36508513 Free Books & Documents.
-
Adapting Safety Plans for Autistic Adults with Involvement from the Autism Community.Autism Adulthood. 2025 May 28;7(3):293-302. doi: 10.1089/aut.2023.0124. eCollection 2025 Jun. Autism Adulthood. 2025. PMID: 40539213
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Nutritional supplementation for hip fracture aftercare in older people.Cochrane Database Syst Rev. 2016 Nov 30;11(11):CD001880. doi: 10.1002/14651858.CD001880.pub6. Cochrane Database Syst Rev. 2016. PMID: 27898998 Free PMC article.
References
-
- Victorian Government. Mental Health and Wellbeing Act 2022 (Act No. 39/2022). 2022. Available from: https://content.legislation.vic.gov.au/sites/default/files/2023-08/22-39.... Accessed January 1, 2025.
-
- Latzer Y, Zohar-Beja A. Compulsory treatment in anorexia nervosa: the case of Israel. Int J Clin Psychiatry Ment Health. 2014;2(2):131–40.
-
- Guillaume S, Gorwood P, Jollant F, Van den Eynde F, Courtet P, Richard-Devantoy S. Impaired decision-making in symptomatic anorexia and bulimia nervosa patients: a meta-analysis. Psychol Med. 2015;45(16):3377–91. - PubMed
-
- Neale J, Hudson LD. Anorexia nervosa in adolescents. Br J Hosp Med. 2020;81(6):1–8. - PubMed
LinkOut - more resources
Full Text Sources
