

Integrating multi-omics and machine learning strategies to explore the "gene-protein-metabolite" network in ischemic heart failure with Qi deficiency and blood stasis syndrome
- PMID: 40671145
- PMCID: PMC12269143
- DOI: 10.1186/s13020-025-01151-9
Integrating multi-omics and machine learning strategies to explore the "gene-protein-metabolite" network in ischemic heart failure with Qi deficiency and blood stasis syndrome
Abstract
Background: Ischemic heart failure (IHF) is a multifaceted syndrome associated with significant mortality and high hospitalization rates globally. According to traditional Chinese medicine (TCM) theory, Qi Deficiency and Blood Stasis (QXXY) Syndrome serves as the pathological basis of IHF. This study aims to investigate the biological basis of QXXY syndrome in IHF patients through an integrated multi-omics approach.
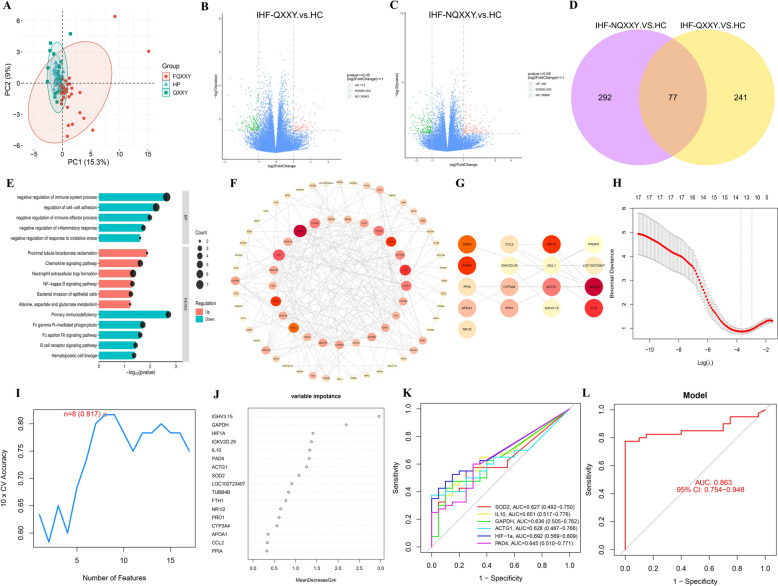
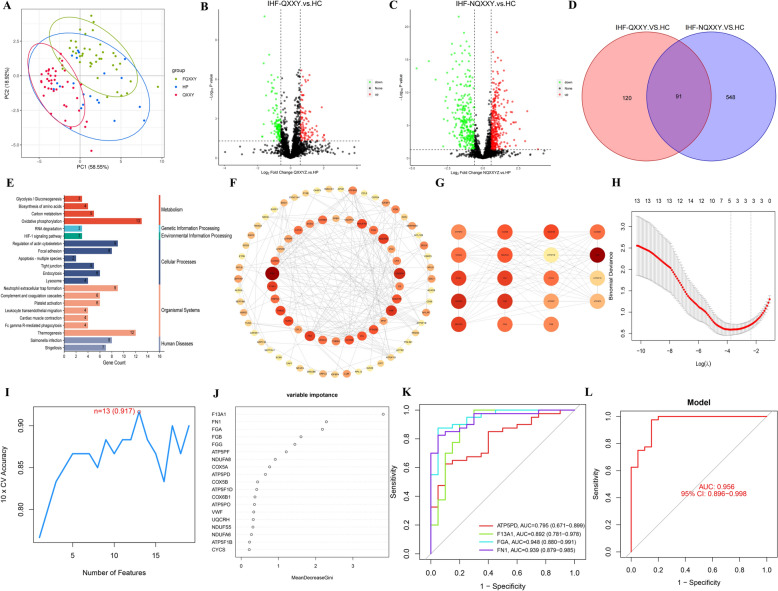
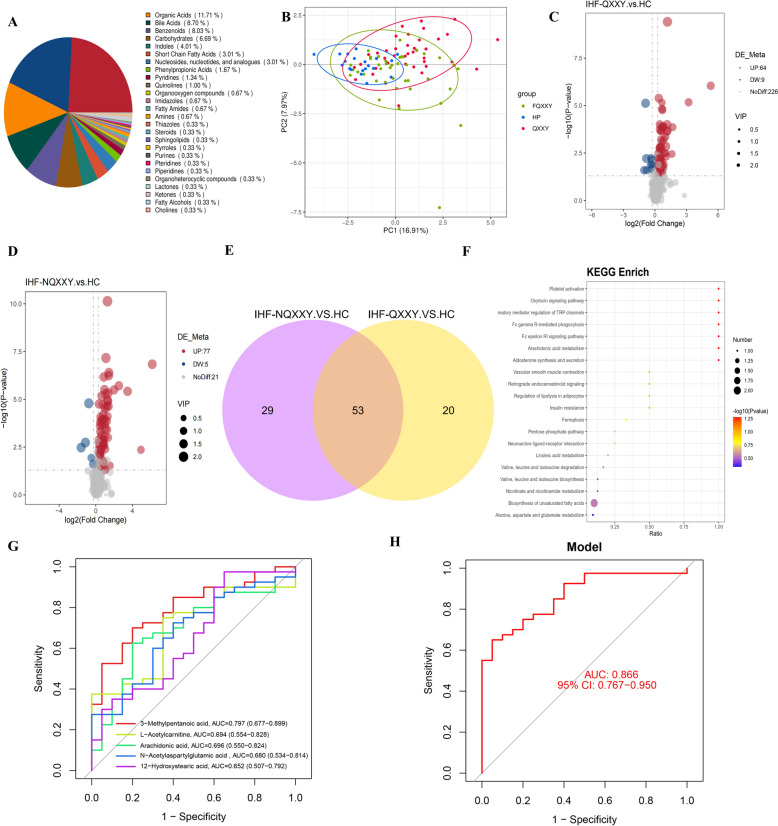
Methods: We enrolled 100 participants, comprising 40 IHF patients with QXXY syndrome (IHF-QXXY), 40 IHF patients without QXXY syndrome, and 20 healthy controls. Utilizing an integrated approach combining RNA sequencing (RNA-seq), data-independent acquisition (DIA) proteomics, and targeted metabolomics, we established a comprehensive "gene-protein-metabolite" network for IHF-QXXY syndrome. Candidate biomarkers were identified through machine learning algorithms and further validated using RT-qPCR and targeted proteomics via intelligent parallel reaction monitoring (iPRM).
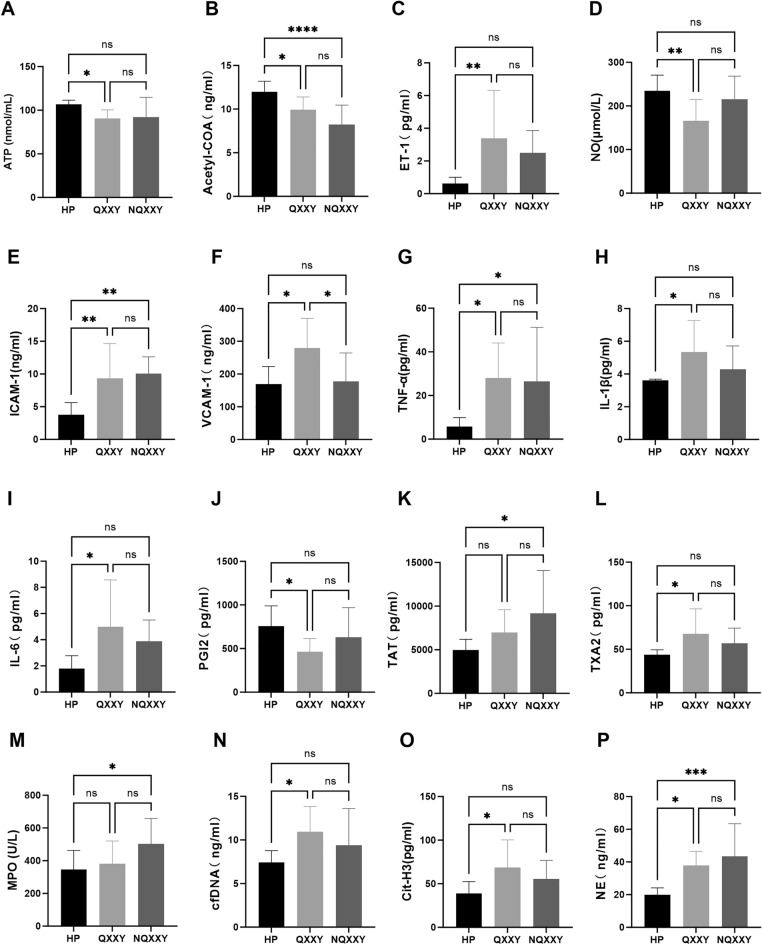
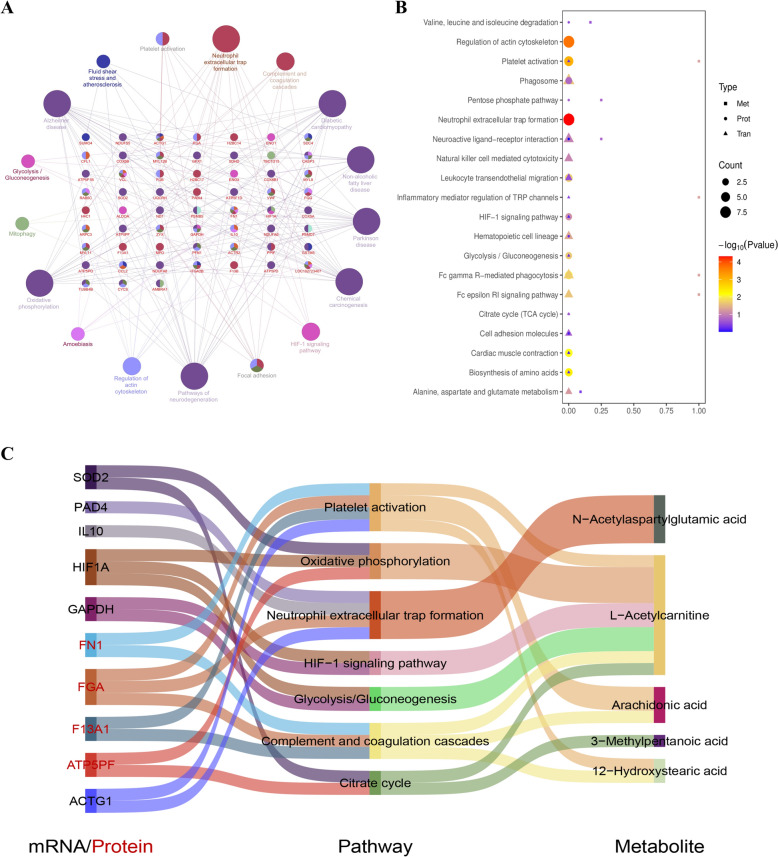
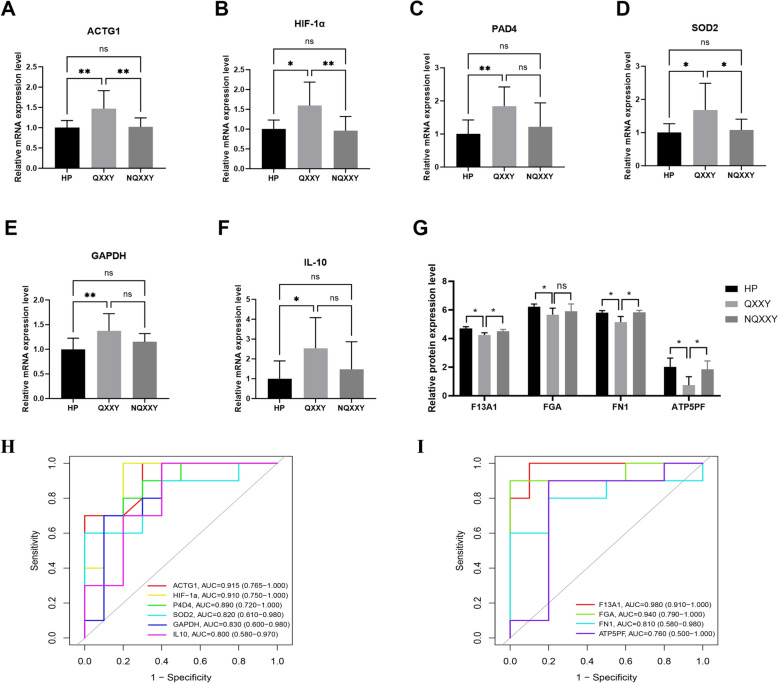
Results: Patients with IHF-QXXY syndrome present with pronounced disruptions in energy metabolism, chronic inflammation, and coagulation abnormalities. The "gene-protein-metabolite" network of IHF-QXXY syndrome comprises six mRNAs, four proteins, and five metabolites. Key pathways involve the activation of neutrophil extracellular traps formation, platelet activation, the HIF-1 signaling pathway, and glycolysis/gluconeogenesis, alongside the suppression of the citrate cycle and oxidative phosphorylation. The key metabolites potentially associated with QXXY syndrome include 3-methylpentanoic acid, arachidonic acid, N-acetylaspartylglutamic acid, L-acetylcarnitine, and 12-hydroxystearic acid. We identified a panel of candidate biomarkers, including HIF-1α, IL10, PAD4, ACTG1, SOD2, GAPDH, FGA, FN1, F13A1, and ATP5PF. This biomarker combination significantly enhanced the diagnostic performance of IHF-QXXY syndrome (AUC > 0.863) and retained high diagnostic accuracy during validation (AUC > 0.75).
Conclusion: This study provides a comprehensive characterization of the molecular features of QXXY syndrome in IHF patients, highlighting key pathways and biomarkers linked to energy metabolism dysregulation, chronic inflammation, and coagulation abnormalities. These findings may provide novel insights and methods for further advancing this research field.
Keywords: Ischemic heart failure; Machine learning; Molecular docking; Multi-omics; Traditional Chinese medicine; Yiqi Huoxue.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study protocol and informed consent form were approved by the Ethics Committee of the First Affiliated Hospital of Henan University of Chinese Medicine (Approval No: 2021HL-178). Consent for publication: Not applicable. Competing interests: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Exploring the biological basis for the identification of different syndromes in ischemic heart failure based on joint multi-omics analysis.Front Pharmacol. 2025 Jul 28;16:1641422. doi: 10.3389/fphar.2025.1641422. eCollection 2025. Front Pharmacol. 2025. PMID: 40792212 Free PMC article.
-
Integrating Gut Microbiome and Metabolomics with Magnetic Resonance Enterography to Advance Bowel Damage Prediction in Crohn's Disease.J Inflamm Res. 2025 Jun 11;18:7631-7649. doi: 10.2147/JIR.S524671. eCollection 2025. J Inflamm Res. 2025. PMID: 40535353 Free PMC article.
-
Exploring the "gene-protein-metabolite" network of coronary heart disease with phlegm and blood stasis syndrome by integrated multi-omics strategy.Front Pharmacol. 2022 Nov 29;13:1022627. doi: 10.3389/fphar.2022.1022627. eCollection 2022. Front Pharmacol. 2022. PMID: 36523490 Free PMC article.
-
Management of urinary stones by experts in stone disease (ESD 2025).Arch Ital Urol Androl. 2025 Jun 30;97(2):14085. doi: 10.4081/aiua.2025.14085. Epub 2025 Jun 30. Arch Ital Urol Androl. 2025. PMID: 40583613 Review.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
References
-
- Savarese G, Becher PM, Lund LH, Seferovic P, Rosano GMC, Coats AJS. Global burden of heart failure: a comprehensive and updated review of epidemiology. Cardiovasc Res. 2023;118(17):3272–87. - PubMed
-
- Khan MS, Shahid I, Bennis A, Rakisheva A, Metra M, Butler J. Global epidemiology of heart failure. Nat Rev Cardiol. 2024;21(10):717–34. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
