

Orthodromic Atrioventricular Reentry Bradycardia and Tachycardia Caused by an Accessory Pathway in Horses
- PMID: 40671630
- PMCID: PMC12268229
- DOI: 10.1111/jvim.70175
Orthodromic Atrioventricular Reentry Bradycardia and Tachycardia Caused by an Accessory Pathway in Horses
Abstract
Background: Accessory pathways (APs) are muscular bundles directly connecting the atria and ventricles, bypassing the atrioventricular (AV) node-His-Purkinje system. Anterograde conduction along the AP results in ventricular preexcitation. A retrograde conducting AP allows ventriculo-atrial (VA) conduction, creating a reentry circuit that mediates orthodromic atrioventricular reentry tachycardia (OAVRT). This condition is well described in humans and small animals, but has not been reported previously in horses.
Objectives: Describe clinical and electrocardiographic findings of horses with retrograde AP conduction and reporte mapping and radiofrequency ablation results in one horse.
Animals: Six horses with retrograde AP conduction.
Methods: Records from six horses with retrograde AP conduction were reviewed.
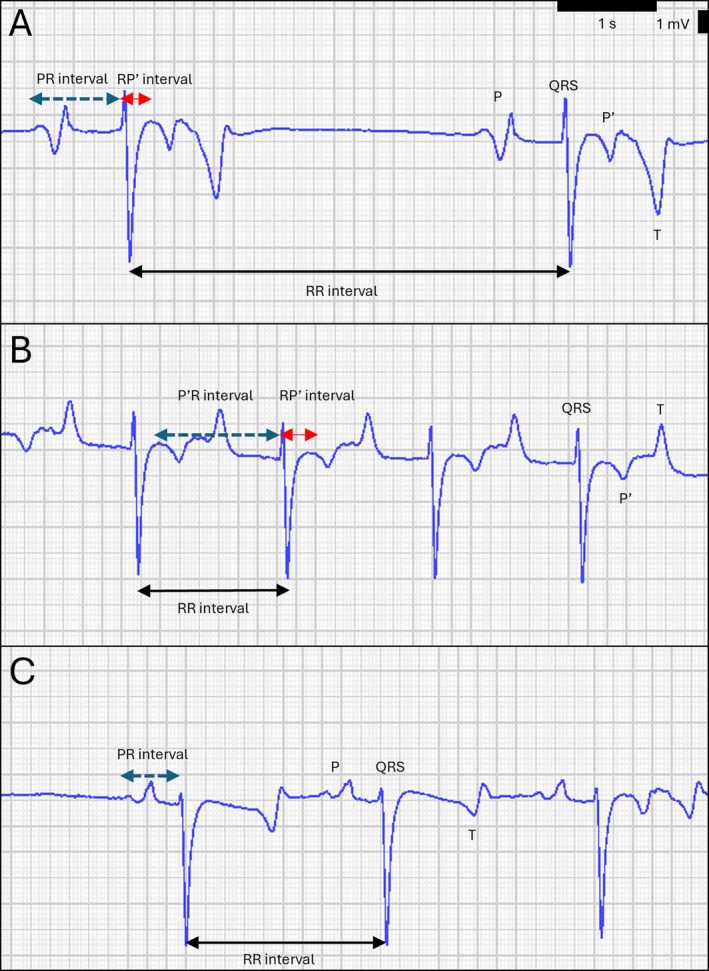
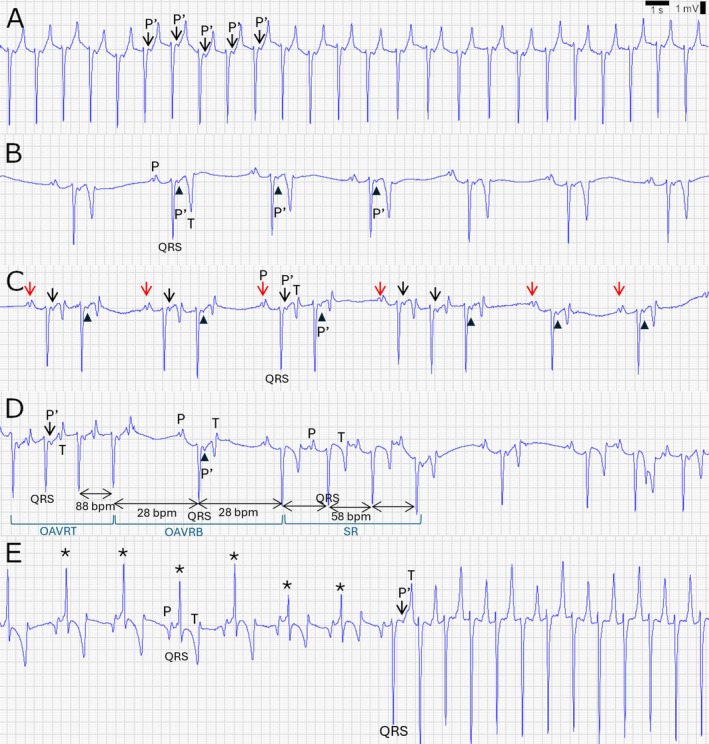
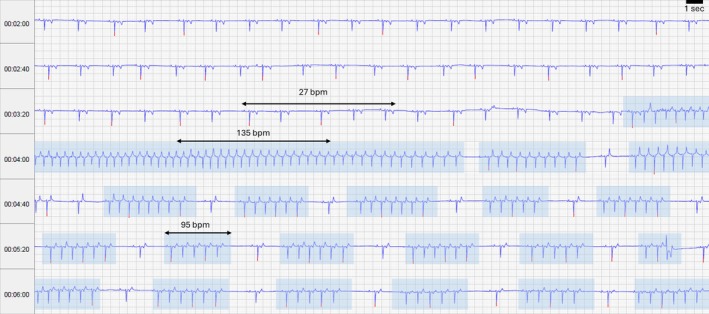
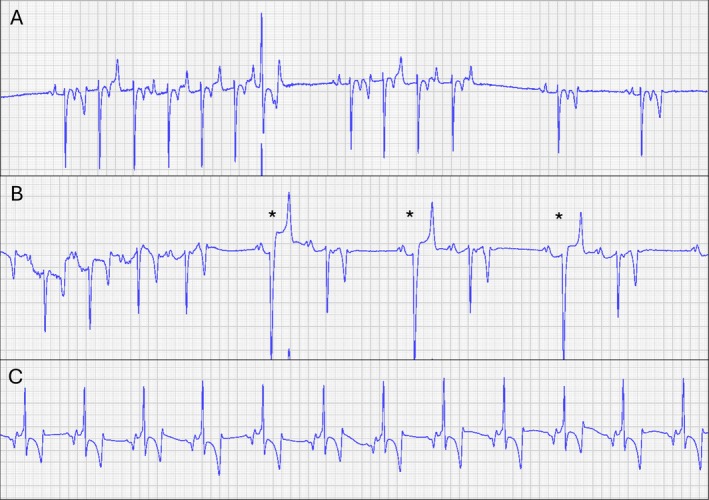
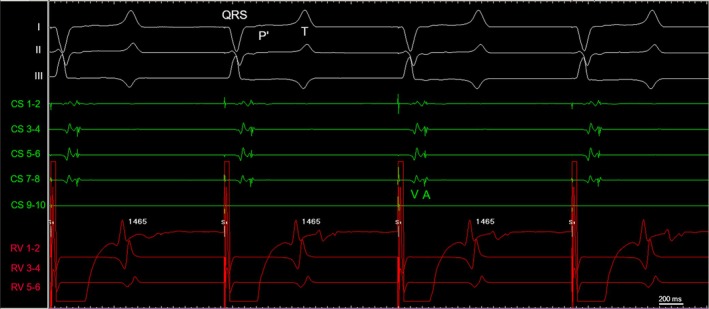
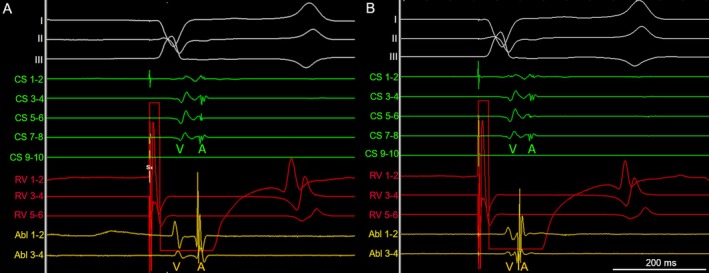
Results: Resting ECGs showed P' waves in the ST segment with fixed coupling intervals to the preceding QRS complexes. In five of six horses, P' waves were conducted back to the ventricles along the AV node, resulting in OAVRT. All horses had episodes where P' waves were blocked at the AV node, which resulted in orthodromic atrioventricular reentry bradycardia (OAVRB). In one horse, the AP conducted bidirectionally resulting in ventricular preexcitation. An electrophysiological study in one horse identified a left-atrial AP insertion by the shortest VA interval. Radiofrequency ablation using an impedance-based mapping system could not eliminate the AP.
Conclusions: Retrograde conducting APs in horses caused OAVRT and OAVRB. APs in horses behaved differently compared to those in humans and dogs. Further research is necessary to elucidate AP behavior, evaluate risk and effect on performance, and assess treatment by ablation.
Keywords: arrhythmias; bypass tract; electrophysiology; equine cardiology.
© 2025 The Author(s). Journal of Veterinary Internal Medicine published by Wiley Periodicals LLC on behalf of American College of Veterinary Internal Medicine.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
Extra-cardiac vagal stimulation: Clinical utility of a novel diagnostic and therapeutic tool in supraventricular tachycardia.J Arrhythm. 2025 Jul 15;41(4):e70134. doi: 10.1002/joa3.70134. eCollection 2025 Aug. J Arrhythm. 2025. PMID: 40666710 Free PMC article.
-
Atrial depolarization electrocardiographic features during orthodromic atrioventricular reciprocating tachycardia mediated by right-sided accessory pathway in the dog.J Vet Cardiol. 2025 Jun 6;61:10-19. doi: 10.1016/j.jvc.2025.06.001. Online ahead of print. J Vet Cardiol. 2025. PMID: 40577935
-
Accessory pathway reciprocating tachycardia.Eur Heart J. 1998 May;19 Suppl E:E13-24, E50-1. Eur Heart J. 1998. PMID: 9717020 Review.
-
Variants of preexcitation--specialized atriofascicular pathways, nodofascicular pathways, and fasciculoventricular pathways: electrophysiologic findings and target sites for radiofrequency catheter ablation.J Cardiovasc Electrophysiol. 1996 Oct;7(10):916-30. doi: 10.1111/j.1540-8167.1996.tb00466.x. J Cardiovasc Electrophysiol. 1996. PMID: 8894934
-
Dual-chamber pacemakers for treating symptomatic bradycardia due to sick sinus syndrome without atrioventricular block: a systematic review and economic evaluation.Health Technol Assess. 2015 Aug;19(65):1-210. doi: 10.3310/hta19650. Health Technol Assess. 2015. PMID: 26293406 Free PMC article.
References
-
- Anderson R. H., Ho S. Y., Gillette P. C., and Becker A. E., “Mahaim, Kent and Abnormal Atrioventricular Conduction,” Cardiovascular Research 31 (1996): 480–491. - PubMed
-
- Issa Z. M. and Zipes D. P., “Typical Atrioventricular Bypass Tracts,” in Clinical Arrhythmiology and Electrophysiology, 3th ed., ed. Issa J. M. (Elsevier, 2019), 599–676.
-
- Santilli R. A., Moïse S., Pariaut R., et al., Electrocardiography the Dog and Cat: Diagnosis of Arrhythmias, 2nd ed. (Edra S.p.A., 2018), 347.
-
- Centurión O. A., Shimizu A., Isomoto S., et al., “Mechanisms for the Genesis of Paroxysmal Atrial Fibrillation in the Wolff—Parkinson—White Syndrome: Intrinsic Atrial Muscle Vulnerability vs. Electrophysiological Properties of the Accessory Pathway,” EP Europace 10 (2008): 294–302. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
