

Global, Regional, and National Burden of Smoking-Related Diseases and Associations With Health Workforce Distribution, 1990-2021: Analysis From the Global Burden of Disease Study 2021
- PMID: 40671918
- PMCID: PMC12263451
- DOI: 10.3389/ijph.2025.1608217
Global, Regional, and National Burden of Smoking-Related Diseases and Associations With Health Workforce Distribution, 1990-2021: Analysis From the Global Burden of Disease Study 2021
Abstract
Objectives: To analyze global trends in smoking-related disease burden from 1990-2021 and examine associations with health workforce distribution across countries.
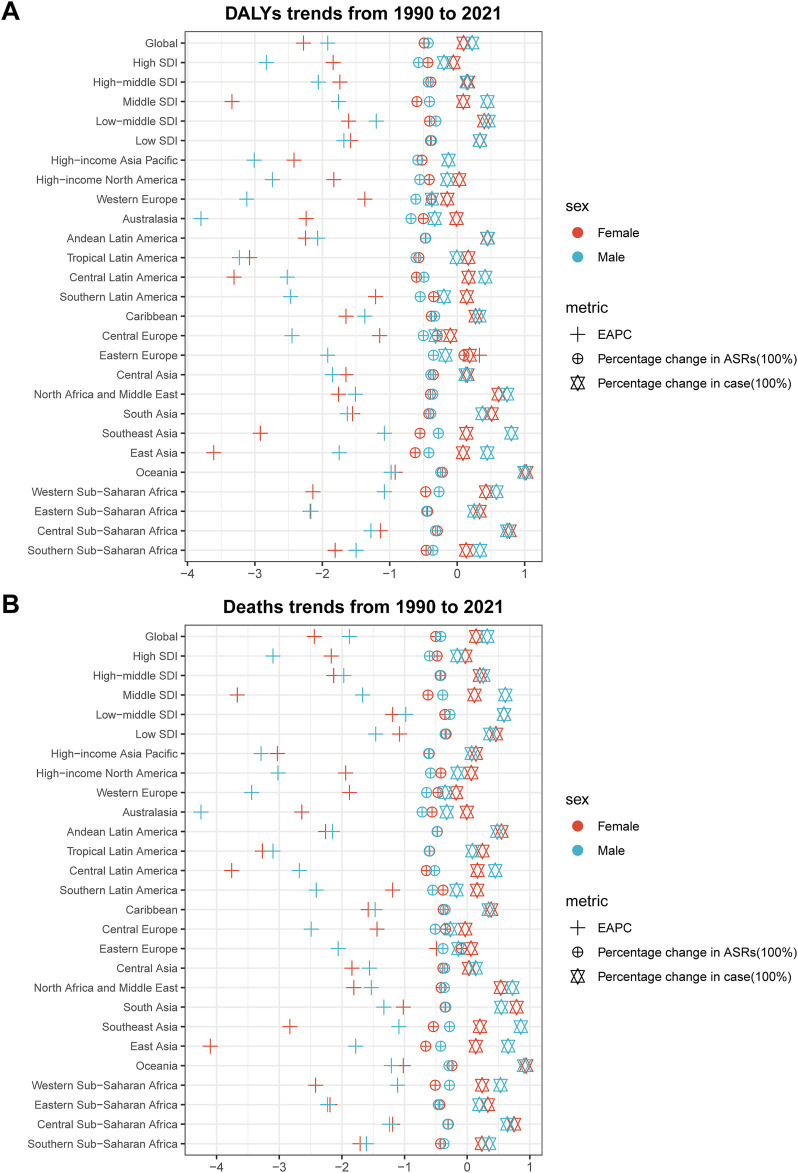
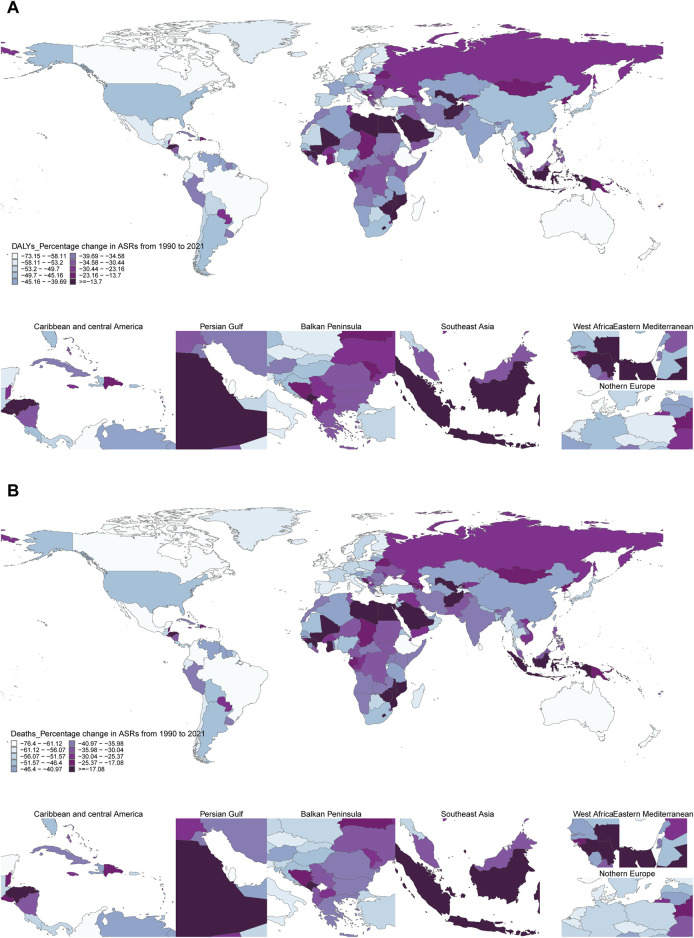
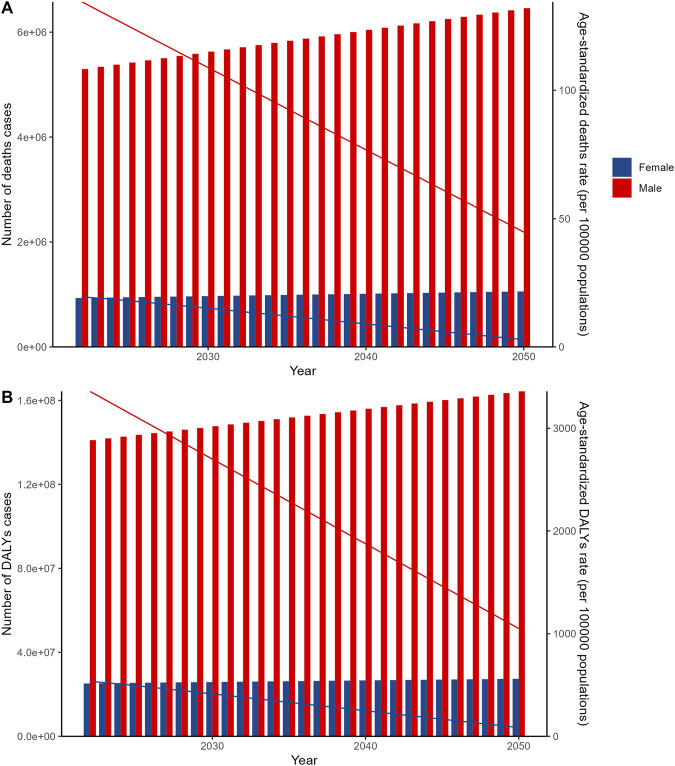
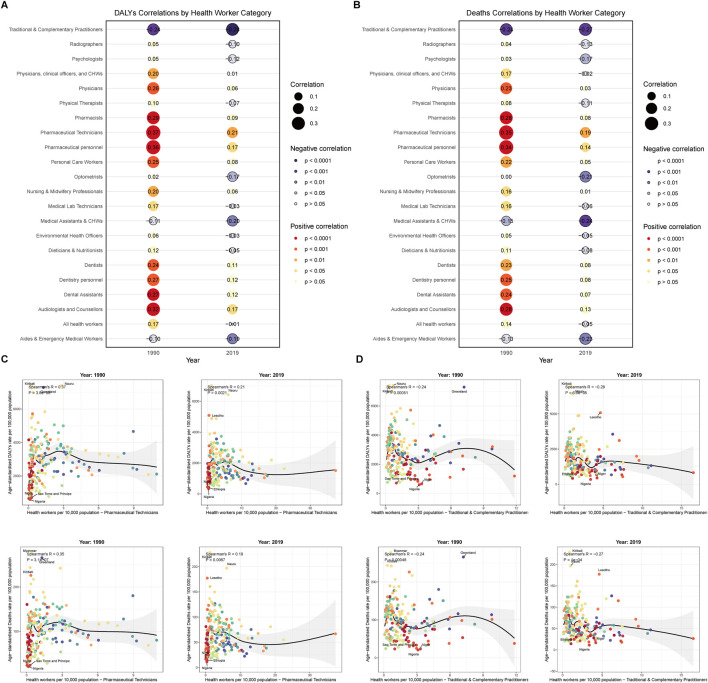
Methods: We analyzed smoking-related deaths and disability-adjusted life years using Global Burden of Disease 2021 data for 204 countries. Age-standardized rates were calculated for 27 geographic regions. Linear regression assessed temporal trends, while autoregressive integrated moving average models projected future burden to 2050. Correlation analyses examined relationships between 22 health workforce categories and disease burden.
Results: Globally, age-standardized death rates from smoking-related diseases increased by 12.3% from 1990-2021, with males showing higher rates than females across all regions. Middle Socio-demographic Index regions exhibited the highest burden. Pharmaceutical technicians demonstrated strong positive correlations with disease burden (r = 0.35-0.37, p < 0.001), while traditional practitioners showed negative correlations (r = -0.24 to -0.28, p < 0.001). Projections indicate continued increases through 2050.
Conclusion: Smoking-related disease burden demonstrates significant geographic and temporal variations, with distinct associations between health workforce composition and disease patterns, highlighting the need for targeted prevention strategies.
Keywords: disease trends; global health burden; health workforce; prevention strategies; smoking-related diseases.
Copyright © 2025 Cai, Chen and Bai.
Conflict of interest statement
The authors declare that they do not have any conflicts of interest.
Figures

Similar articles
-
Global pattern, trend and cross-country inequalities of inguinal, femoral, and abdominal hernia among individuals aged 60 and above from 1990 to 2021 and projections until 2040: a population-based study.Surg Endosc. 2025 Jul;39(7):4335-4344. doi: 10.1007/s00464-025-11810-5. Epub 2025 May 28. Surg Endosc. 2025. PMID: 40437076
-
Ambient versus household PM2.5 exposure and socioeconomic disparities in intracerebral hemorrhage burden: a 32-year global analysis (1990-2021) with projections to 2050.Front Public Health. 2025 Jun 18;13:1615934. doi: 10.3389/fpubh.2025.1615934. eCollection 2025. Front Public Health. 2025. PMID: 40606082 Free PMC article.
-
Global regional and national burden of intracerebral hemorrhage between 1990 and 2021.Sci Rep. 2025 Jan 29;15(1):3624. doi: 10.1038/s41598-025-88017-0. Sci Rep. 2025. PMID: 39880918 Free PMC article.
-
Reducible burden of laryngeal cancer in men aged 50 and older attributable to smoking and alcohol use: insights from the global burden of disease study 2021.Front Public Health. 2025 Jun 9;13:1577138. doi: 10.3389/fpubh.2025.1577138. eCollection 2025. Front Public Health. 2025. PMID: 40552237 Free PMC article.
-
Global, Regional, and National Burden and Trends of Soft Tissue and Other Extraosseous Sarcomas From 1990 to 2021.Cancer Control. 2025 Jan-Dec;32:10732748251355841. doi: 10.1177/10732748251355841. Epub 2025 Jun 28. Cancer Control. 2025. PMID: 40580032 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical