

Giant Cell Arteritis Presenting As Pyrexia of Unknown Origin: Diagnosis Made by Bilateral Periluminal Dark Halo Sign on Color Doppler Ultrasound
- PMID: 40672026
- PMCID: PMC12266085
- DOI: 10.7759/cureus.86134
Giant Cell Arteritis Presenting As Pyrexia of Unknown Origin: Diagnosis Made by Bilateral Periluminal Dark Halo Sign on Color Doppler Ultrasound
Abstract
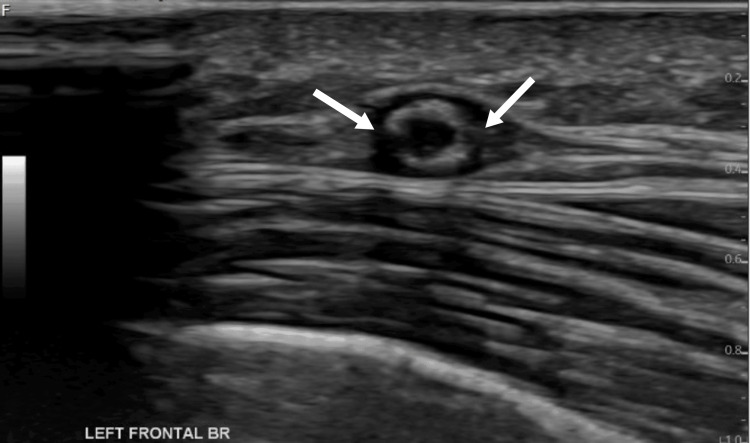
Giant cell arteritis (GCA), a vasculitis of medium- and large-sized arteries, frequently manifests with symptoms such as headaches, soreness in the scalp, and vision abnormalities. Pyrexia is an uncommon symptom and can cause a delay in diagnosis. We describe a 76-year-old woman of Chinese ethnicity who did not exhibit the typical clinical signs of GCA but instead presented with a generalized lethargy, nausea, dizziness, and a persistent fever. Numerous tests, including autoimmune, neoplastic, and viral workups, came up negative. Pyrexia did not settle despite using broad-spectrum antibiotics. A temporal artery Doppler ultrasound was performed to assess the condition further, as inflammatory markers (erythrocyte sedimentation rate, ESR, and C-reactive protein) remained high. The ultrasound Doppler results showed bilateral halo signs that are very specific for GCA. Upon starting corticosteroid treatment, there was a rapid improvement in fever and ESR. This case underscores the importance of considering GCA as a differential diagnosis for pyrexia of unknown origin, particularly in the elderly. It highlights the utility of temporal artery ultrasound in facilitating timely diagnosis in atypical cases.
Keywords: giant cell arteritis; halo sign; pyrexia of unknown origin; temporal artery ultrasound; vasculitis.
Copyright © 2025, Siddique et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures





Similar articles
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Ultrasound vs. biopsy in diagnosing giant cell arteritis in the Royal Victoria Eye and Ear Hospital, Dublin: a clinical comparison.Ir J Med Sci. 2025 Aug 9. doi: 10.1007/s11845-025-04063-7. Online ahead of print. Ir J Med Sci. 2025. PMID: 40782233
-
Tocilizumab for giant cell arteritis.Cochrane Database Syst Rev. 2022 May 13;5(5):CD013484. doi: 10.1002/14651858.CD013484.pub3. Cochrane Database Syst Rev. 2022. PMID: 35560150 Free PMC article.
-
Polymyalgia Rheumatica and Giant Cell Arteritis: A Systematic Review.JAMA. 2016 Jun 14;315(22):2442-58. doi: 10.1001/jama.2016.5444. JAMA. 2016. PMID: 27299619
References
-
- Giant cell arteritis presenting as PUO. Santhanam S, Mani SK. https://pubmed.ncbi.nlm.nih.gov/28799318/ J Assoc Physicians India. 2017;65:107–108. - PubMed
-
- The clinical benefit of imaging in the diagnosis and treatment of giant cell arteritis. Berger CT, Sommer G, Aschwanden M, Staub D, Rottenburger C, Daikeler T. Swiss Med Wkly. 2018;148:0. - PubMed
-
- Diagnostic validity of Doppler ultrasound in giant cell arteritis. Aranda-Valera IC, García Carazo S, Monjo Henry I, De Miguel Mendieta E. https://pubmed.ncbi.nlm.nih.gov/28244857/ Clin Exp Rheumatol. 2017;35 Suppl 103:123–127. - PubMed
-
- Role of ultrasonography in the diagnosis of temporal arteritis. Ball EL, Walsh SR, Tang TY, Gohil R, Clarke JM. Br J Surg. 2010;97:1765–1771. - PubMed
-
- 2022 American College of Rheumatology/EULAR classification criteria for giant cell arteritis. Ponte C, Grayson PC, Robson JC, et al. Arthritis Rheumatol. 2022;74:1881–1889. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous