

Clinical and endoscopic characteristics of colorectal sessile serrated lesion with dysplasia: a single-center cross-sectional comparative study
- PMID: 40672066
- PMCID: PMC12261020
- DOI: 10.21037/jgo-2024-901
Clinical and endoscopic characteristics of colorectal sessile serrated lesion with dysplasia: a single-center cross-sectional comparative study
Abstract
Background: The precancerous lesion of colorectal cancer (CRC), colorectal sessile serrated lesion (SSL), takes an average of 15 years to germinate from no cell dysplasia to CRC, and 2 years for SSL with dysplasia (SSL-D). To date, the impacts of endoscopic and pathological features of SSL and SSL-D on the development of dysplasia remain unclear. In this study, we explored these impacts, striving to provide reference for its classification, detection, and diagnosis.
Methods: Retrospectively, a cross-sectional analysis was conducted to compare 414 SSL and 59 SSL-D, which had been diagnosed under colonoscopy in the Affiliated Drum Tower Hospital of Nanjing University.
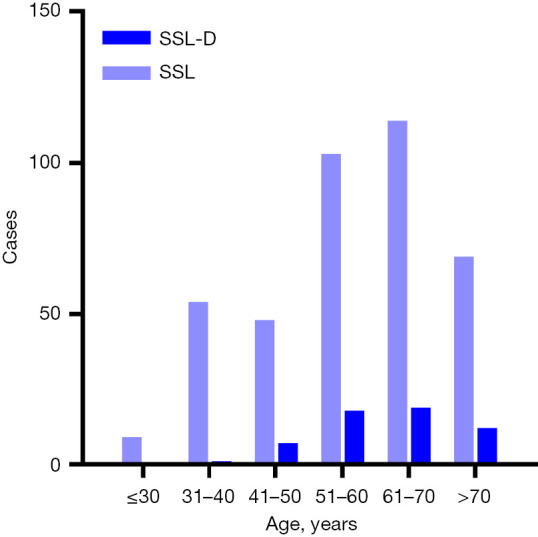
Results: A total of 454 participants were enrolled with a mean age of 58.43±13.94 years and a male-to-female ratio of 0.91:1. There were significant differences between the SSL and SSL-D groups in the gender distribution (P=0.044). The proportion of patients with hypertension (33.33% vs. 17.13%, P=0.004) was higher in the SSL-D group. Significantly higher indexes in lipid metabolism were observed in the SSL-D group. SSL-D had a greater number of lesions ≥10 mm (86.44% vs. 57.00%, P<0.001), 0-IIa morphology (55.93% vs. 41.55%, P=0.049), and kermesinus surface (22.03% vs. 7.49%, P<0.001).
Conclusions: Female SSL patients with a history of hypertension are more prone to developing into dysplasia, whereas morphological discriminations between SSL and SSL-D are vague. Lipid metabolism might have certain impact on the germination of SSL to SSL-D. Studies with larger sample sizes are warranted.
Keywords: Sessile serrated lesion (SSL); colorectal cancer (CRC); dysplasia; endoscopic features; lipid metabolism.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jgo.amegroups.com/article/view/10.21037/jgo-2024-901/coif). The authors have no conflicts of interest to declare.
Figures

Similar articles
-
Inflammatory bowel disease-associated serrated lesions with dysplasia are frequently associated with advanced neoplasia: supporting a unified classification approach.Histopathology. 2025 Sep;87(3):408-423. doi: 10.1111/his.15448. Epub 2025 Mar 19. Histopathology. 2025. PMID: 40104985
-
Whole-Exome Sequencing Analysis of Inflammatory Bowel Disease-Associated Serrated Dysplasia.Int J Mol Sci. 2025 Jun 13;26(12):5704. doi: 10.3390/ijms26125704. Int J Mol Sci. 2025. PMID: 40565166 Free PMC article.
-
Strategies for detecting colon cancer in patients with inflammatory bowel disease.Cochrane Database Syst Rev. 2017 Sep 18;9(9):CD000279. doi: 10.1002/14651858.CD000279.pub4. Cochrane Database Syst Rev. 2017. PMID: 28922695 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Strategies for detecting colon cancer and/or dysplasia in patients with inflammatory bowel disease.Cochrane Database Syst Rev. 2006 Apr 19;(2):CD000279. doi: 10.1002/14651858.CD000279.pub3. Cochrane Database Syst Rev. 2006. Update in: Cochrane Database Syst Rev. 2017 Sep 18;9:CD000279. doi: 10.1002/14651858.CD000279.pub4. PMID: 16625534 Updated.
References
LinkOut - more resources
Full Text Sources