

FAT1 mutation-related signature predicts survival risk and tumor immunogenicity in lung adenocarcinoma
- PMID: 40672387
- PMCID: PMC12263358
- DOI: 10.3389/fgene.2025.1466484
FAT1 mutation-related signature predicts survival risk and tumor immunogenicity in lung adenocarcinoma
Abstract
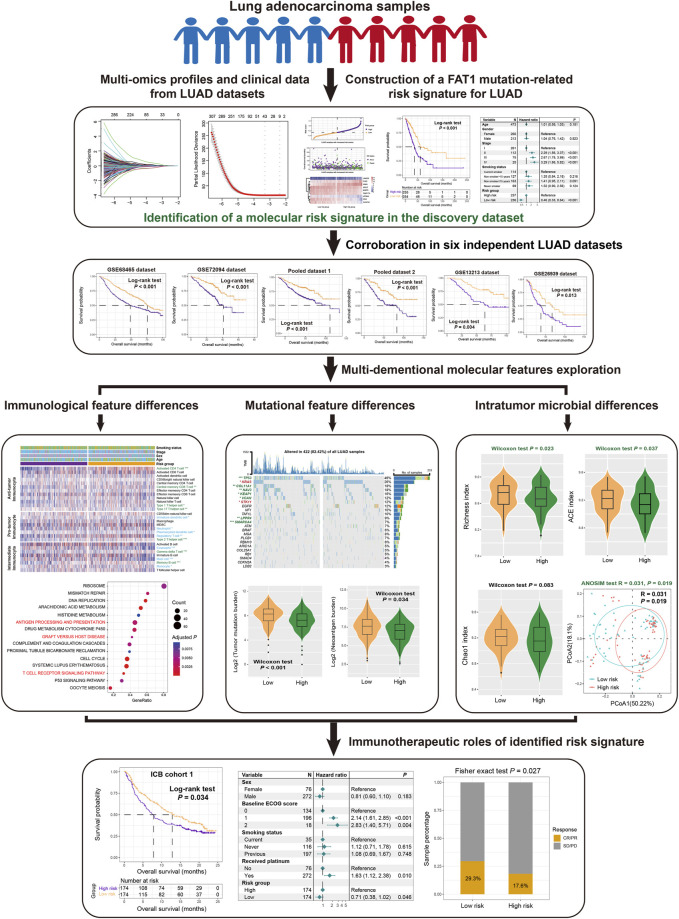
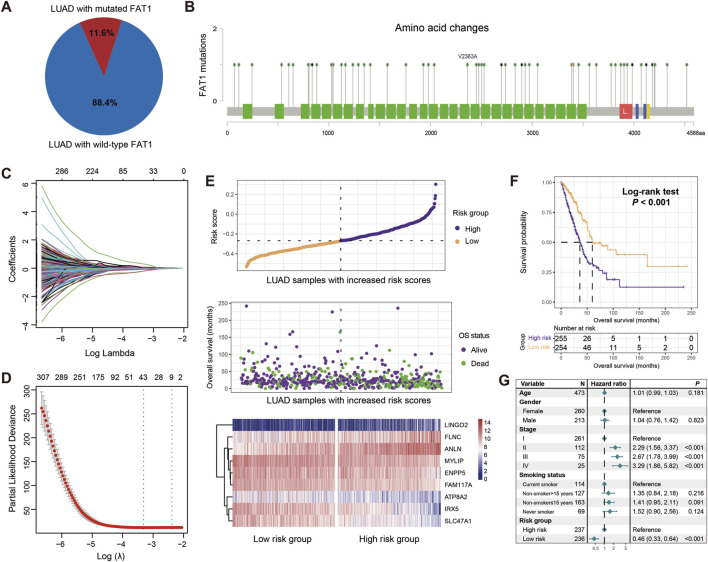
Background: FAT atypical cadherin 1 (FAT1) is a well-known tumor regulator that plays a crucial role in multiple cancer signaling pathways. Its mutations have been linked to tumor progression and immune regulation in various cancers, including lung adenocarcinoma (LUAD). In this study, we aim to identify a FAT1 mutation-related transcriptomic risk signature to assess the survival risks and immune status of LUAD patients.
Methods: A total of 2528 LUAD samples, which included both gene expression profiles and clinicopathologic data, were collected from 12 datasets. Additionally, two datasets treated with immunotherapies were also included to investigate the therapeutic effects.
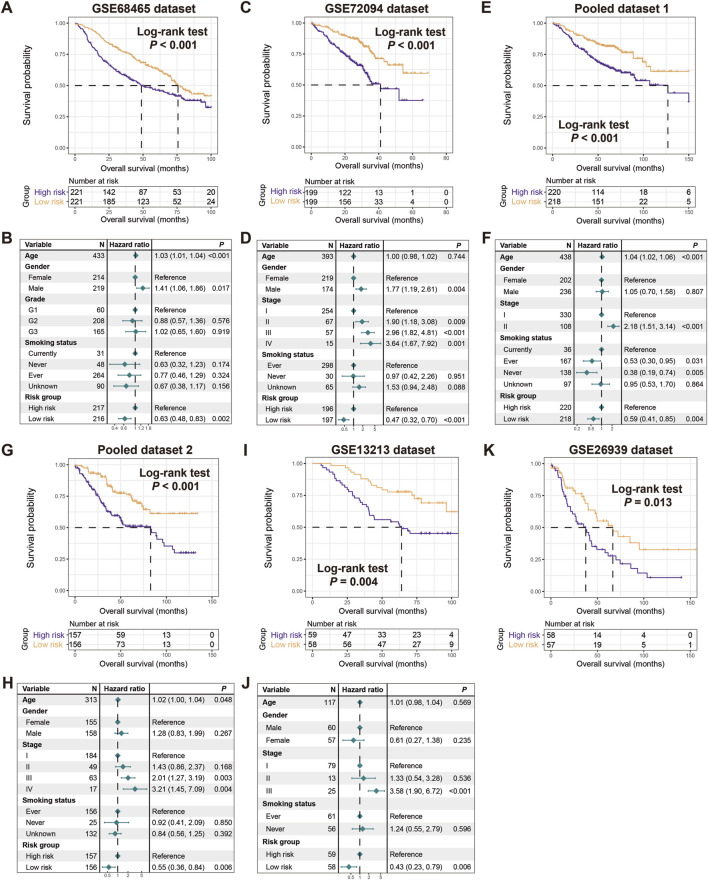
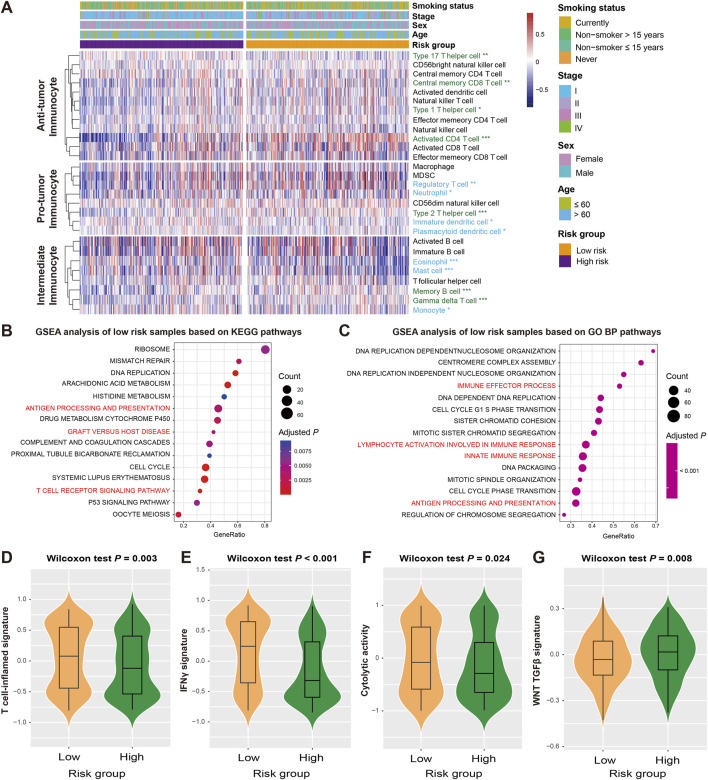
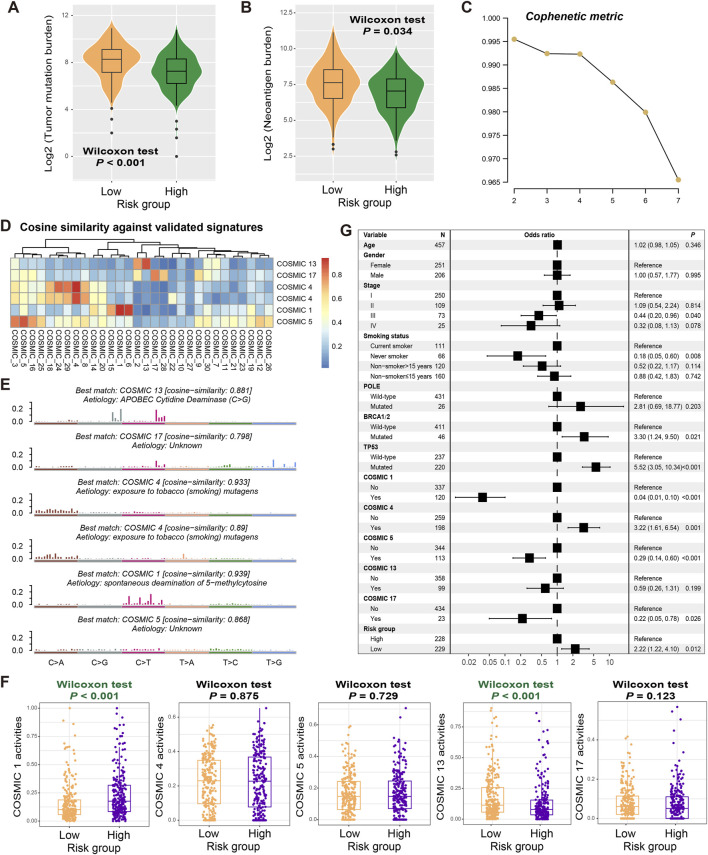
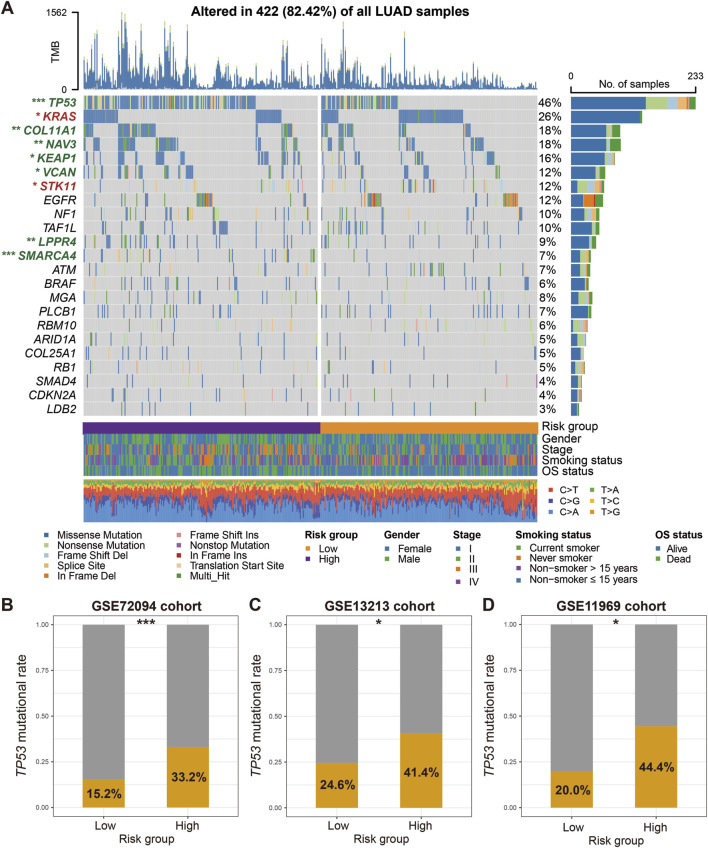
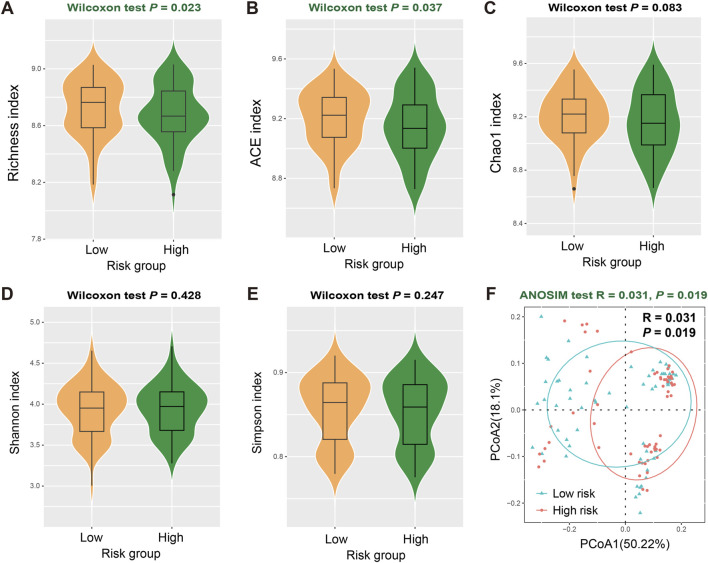
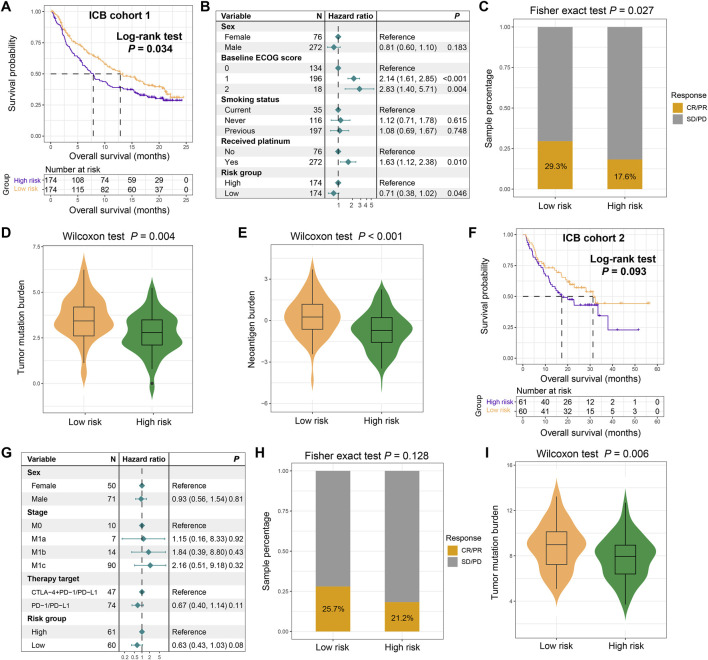
Results: We constructed a FAT1 mutation molecular signature based on 9 relevant genes. LUAD patients with low-risk scores demonstrated a more favorable prognosis compared to those with high-risk scores, which is corroborated by 6 additional independent datasets. Further immunological, mutational, and intratumor microbial analyses reveal that increased infiltration of immune effector cells, increased mutational burden, specific mutational signatures (such as age and APOBEC associated), mutations in driver genes (e.g., TP53, KEAP1, NAV3, and SMARCA4), and increased microbial α/β diversities are present in the low-risk LUAD patients. Based on the immunotherapeutic patients, an improved immune checkpoint blockade treatment prognosis and an elevated response rate are also observed in the low-risk signature group.
Conclusion: In summary, Our identified FAT1 mutation-related risk signature shows potential for assessing LUAD clinical outcomes, tumor immunogenicity, and immunotherapy effectiveness, providing valuable insights for LUAD clinical practice.
Keywords: FAT1 mutation signature; immune treatment; lung adenocarcinoma; prognostic indicators; survival risk; tumor immunogenicity.
Copyright © 2025 Gao, Wang, Xu, Wang, Zhang, Wang and Ren.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Molecular subtypes of lung adenocarcinoma patients for prognosis and therapeutic response prediction with machine learning on 13 programmed cell death patterns.J Cancer Res Clin Oncol. 2023 Oct;149(13):11351-11368. doi: 10.1007/s00432-023-05000-w. Epub 2023 Jun 28. J Cancer Res Clin Oncol. 2023. PMID: 37378675 Free PMC article.
-
Comprehensive analysis of co-expressed genes with TDP-43: prognostic and therapeutic potential in lung adenocarcinoma.J Cancer Res Clin Oncol. 2024 Jan 28;150(2):44. doi: 10.1007/s00432-023-05554-9. J Cancer Res Clin Oncol. 2024. PMID: 38281298 Free PMC article.
-
Prognostic and onco-immunological value of immune-related eRNAs-driven genes in lung adenocarcinoma.J Cancer Res Clin Oncol. 2024 Apr 11;150(4):188. doi: 10.1007/s00432-024-05687-5. J Cancer Res Clin Oncol. 2024. PMID: 38602568 Free PMC article.
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.Health Technol Assess. 2006 Sep;10(34):iii-iv, ix-xi, 1-204. doi: 10.3310/hta10340. Health Technol Assess. 2006. PMID: 16959170
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous