

Why do older adults hesitate to get the flu vaccine? A cross-sectional study on vaccine hesitancy in the post-COVID-19 era
- PMID: 40672922
- PMCID: PMC12265952
- DOI: 10.3389/fpubh.2025.1603091
Why do older adults hesitate to get the flu vaccine? A cross-sectional study on vaccine hesitancy in the post-COVID-19 era
Abstract
Objectives: To investigate the determinants of influenza vaccine hesitancy (VH) among older adults in Shanghai, China, using the 3Cs model (confidence, complacency, and convenience) and vaccine literacy (VL) framework. This study also explored the potential effect of COVID-19 vaccine hesitancy on influenza vaccine attitudes in the post-COVID-19 era.
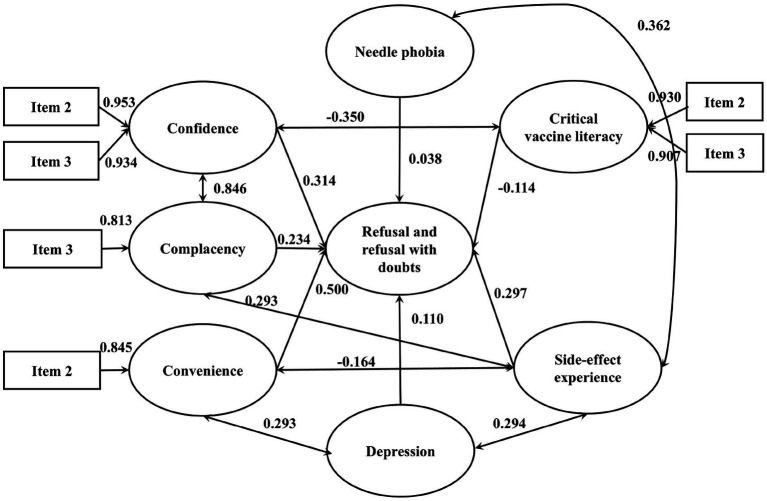
Methods: We conducted a community-based cross-sectional study from January to June 2024 in Shanghai, China, involving 1,300 adults aged ≥60 years. Participants were recruited through stratified random sampling. Inclusion criteria were: community-dwelling adults aged ≥60 years in Xuhui District. Multinomial logistic regression models were used to identify predictors of vaccine hesitancy, adjusting for sociodemographic variables, self-reported health status and self-report vaccination experiences. Structural equation modeling (SEM) was employed to examine the underlying factors contributing to vaccine hesitancy and quantify their interrelationships.
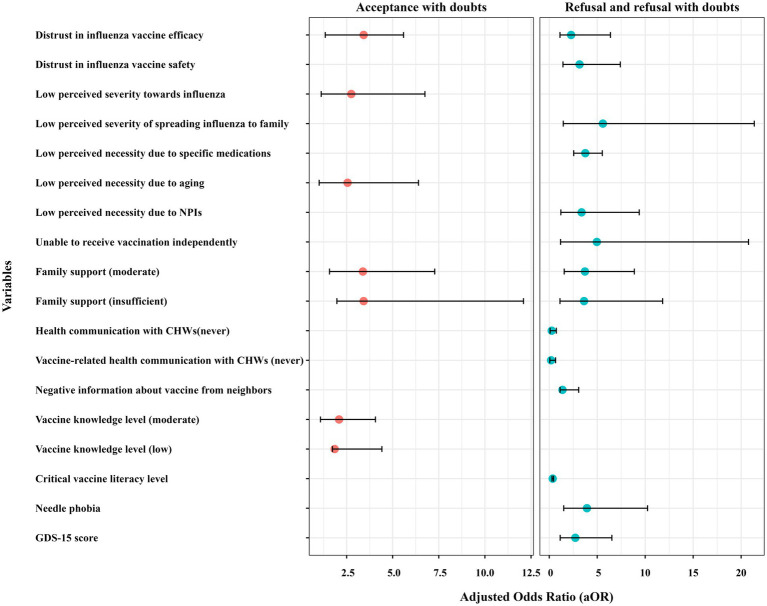
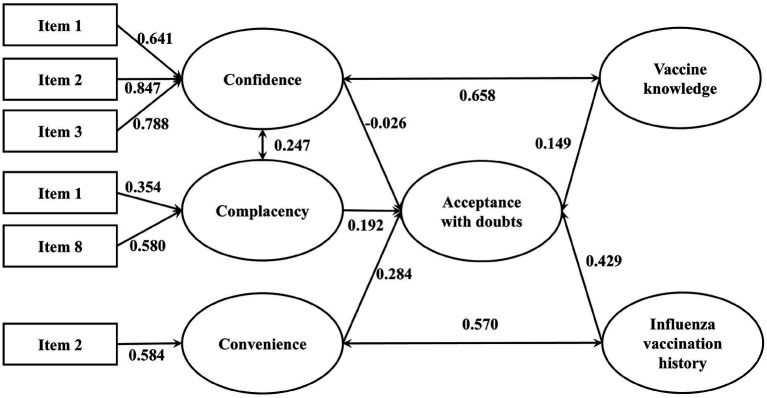
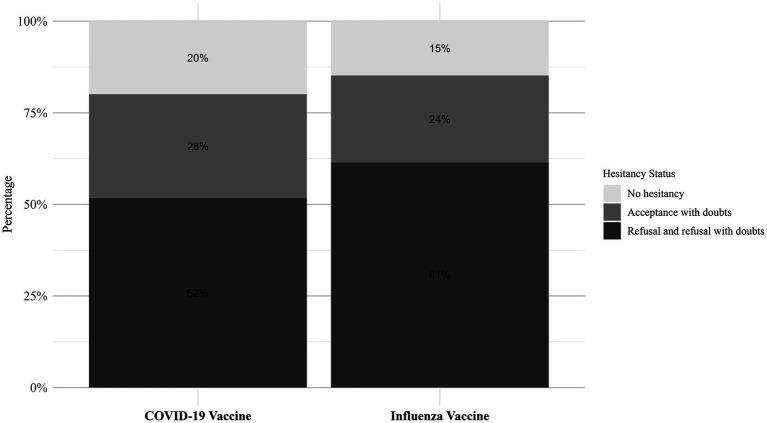
Results: A high proportion (85.2%) of participants exhibited influenza vaccine hesitancy, with 16.2% being complete refusers. Key predictors of hesitancy included distrust in vaccine efficacy (adjusted Odds Ratio [aOR] = 2.28 for refusal), low perceived influenza severity (aOR = 5.59 for refusal), and overreliance on non-pharmaceutical interventions (NPIs) (aOR = 3.37 for refusal) and influenza-specific medication (aOR = 3.76). Limited health communication with community health workers (CHWs) and low family support significantly amplified refusal risks (aOR = 3.63). Higher vaccine knowledge reduced hesitancy (aOR = 1.85), though paradoxically, higher critical vaccine literacy correlated with refusal tendencies (aOR = 0.36). Significant standardized estimated coefficient (β) were observed between confidence and complacency (β = 0.846), side-effect experience and complacency (β = 0.293), side-effect experience and depression (β = 0.294), convenience and depression (β = 0.293), and side-effect experience and needle phobia (β = 0.362).
Conclusion: Vaccine confidence deficits and complacency regarding influenza severity are major drivers of hesitancy in older adults. This hesitancy is further exacerbated by COVID-19 vaccine skepticism and nuanced aspects of vaccine literacy. System-level interventions should integrate proactive vaccine counseling into routine care, strengthen family engagement in immunization decisions, and develop misinformation-resilient vaccine literacy programs specifically tailored for this vulnerable population.
Keywords: 3Cs model; influenza; older adult; vaccination hesitancy; vaccine literacy.
Copyright © 2025 Wang, Wen, Wu, Cui, Shen, Hu, Zeng and Tang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
From institutional trust to digital literacy: Socioeconomic and political determinants of COVID-19 vaccine hesitancy among Czech adults based on a national panel survey.Hum Vaccin Immunother. 2025 Dec;21(1):2533639. doi: 10.1080/21645515.2025.2533639. Epub 2025 Jul 15. Hum Vaccin Immunother. 2025. PMID: 40665470 Free PMC article.
-
[Hesitancy and Refusal of the COVID-19 Vaccine Among Healthcare Professionals: A Cross-Sectional Study in a Portuguese Hospital].Acta Med Port. 2025 Apr 1;38(4):217-227. doi: 10.20344/amp.22540. Epub 2025 Apr 1. Acta Med Port. 2025. PMID: 40185134 Portuguese.
-
Parental hesitancy on COVID-19 vaccination of children under the age of 16: A cross-sectional mixed-methods study among factory workers.PLoS One. 2025 Jun 26;20(6):e0327056. doi: 10.1371/journal.pone.0327056. eCollection 2025. PLoS One. 2025. PMID: 40569977 Free PMC article.
-
Acceptance-Hesitancy of COVID-19 Vaccination and Factors Affecting It in Adults: Systematic Review Study.Immun Inflamm Dis. 2024 Nov;12(11):e70076. doi: 10.1002/iid3.70076. Immun Inflamm Dis. 2024. PMID: 39570098 Free PMC article.
-
Vaccines for preventing infections in adults with haematological malignancies.Cochrane Database Syst Rev. 2025 May 21;5(5):CD015530. doi: 10.1002/14651858.CD015530.pub2. Cochrane Database Syst Rev. 2025. PMID: 40396505 Review.
References
-
- Lafond KE, Porter RM, Whaley MJ, Suizan Z, Ran Z, Aleem MA, et al. Global burden of influenza-associated lower respiratory tract infections and hospitalizations among adults: a systematic review and meta-analysis. PLoS Med. (2021) 18:e1003550. doi: 10.1371/journal.pmed.1003550, PMID: - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical