

The lifetime accumulation of multimorbidity and its influence on dementia risk: a UK Biobank study
- PMID: 40672935
- PMCID: PMC12266833
- DOI: 10.1093/braincomms/fcaf222
The lifetime accumulation of multimorbidity and its influence on dementia risk: a UK Biobank study
Abstract
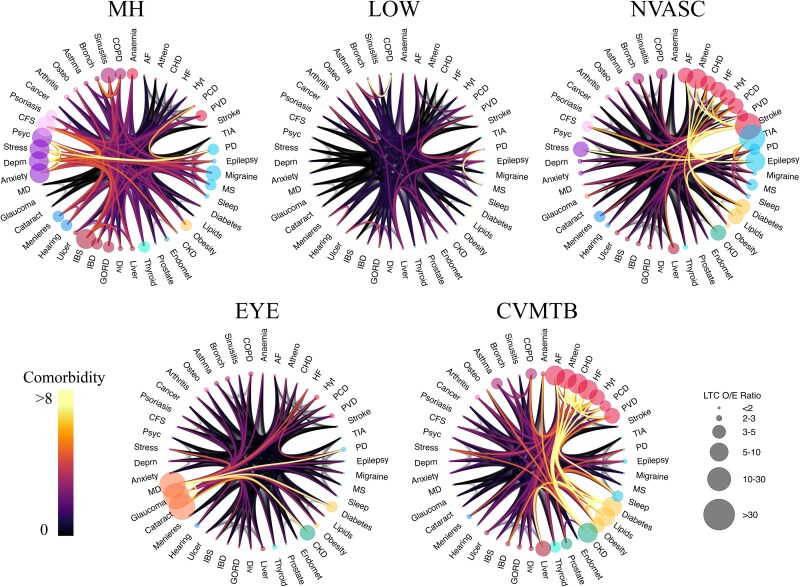
The number of people living with dementia worldwide is projected to reach 150 million by 2050, making prevention a crucial priority for health services. The co-occurrence of two or more chronic health conditions, termed multimorbidity, occurs in up to 80% of dementia patients, making multimorbidity an important risk factor for dementia. However, we lack an understanding of the specific health conditions, and their age of onset, that drive the link between multimorbidity and dementia. Using data from 282 712 participants of the UK Biobank, we defined the sequential patterns of accumulation of 46 chronic conditions over the life course. By grouping individuals based on their life history of chronic illness, we show here that the risk of incident dementia can be stratified by both the type and timing of their accumulated chronic conditions. We identified several distinct clusters of multimorbidity throughout the lifespan (cardiometabolic, mental health, neurovascular, peripheral vascular, eye diseases and low/no multimorbidity). We observed that the odds of developing dementia varied based on when these comorbidities were diagnosed. Until midlife (age 55), the accumulation of cardiometabolic conditions, such as coronary heart disease, atrial fibrillation, and diabetes, was most strongly associated with dementia risk. However, from 55 to 70 years, the accumulation of mental health conditions, such as anxiety and depression, as well as neurovascular conditions, such as stroke and transient ischaemic attack, was associated with an over 2-fold increase in dementia risk compared with low multimorbidity. Importantly, individuals who continuously and sequentially accumulate cardiometabolic, mental health, and neurovascular conditions were at greatest risk. The age-dependent role of multimorbidity in predicting dementia risk could be used for early stratification of individuals into high- and low-risk groups and could inform targeted prevention strategies based on a person's prior history of chronic disease.
Keywords: cluster analysis; dementia; multimorbidity; risk stratification.
© The Author(s) 2025. Published by Oxford University Press on behalf of the Guarantors of Brain.
Conflict of interest statement
The authors report no competing interests.
Figures





References
-
- Winblad B, Amouyel P, Andrieu S, et al. Defeating Alzheimer’s disease and other dementias: A priority for European science and society. Lancet Neurol. 2016;15(5):455–532. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources