

Itaconate suppresses neonatal intestinal inflammation via metabolic reprogramming of M1 macrophage
- PMID: 40673634
- PMCID: PMC12268792
- DOI: 10.1002/ctm2.70419
Itaconate suppresses neonatal intestinal inflammation via metabolic reprogramming of M1 macrophage
Abstract
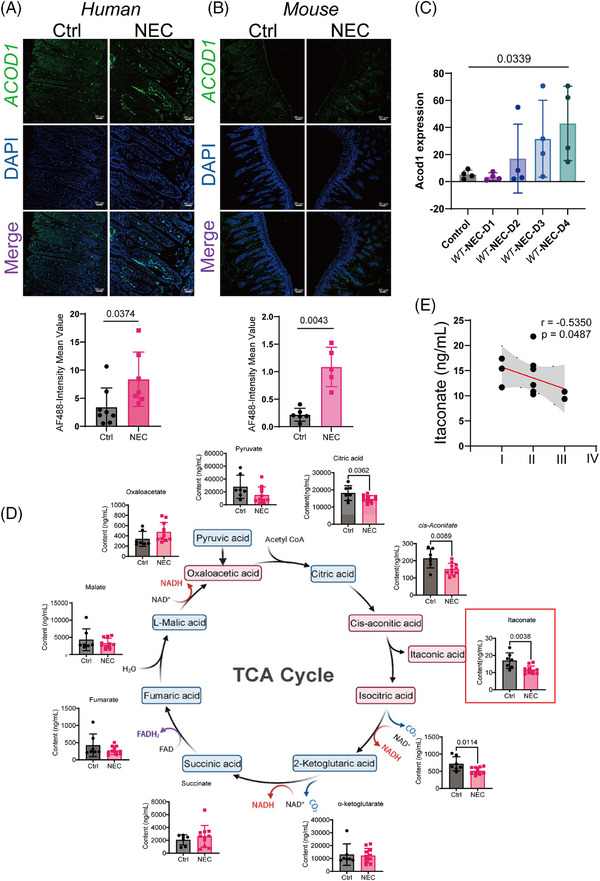
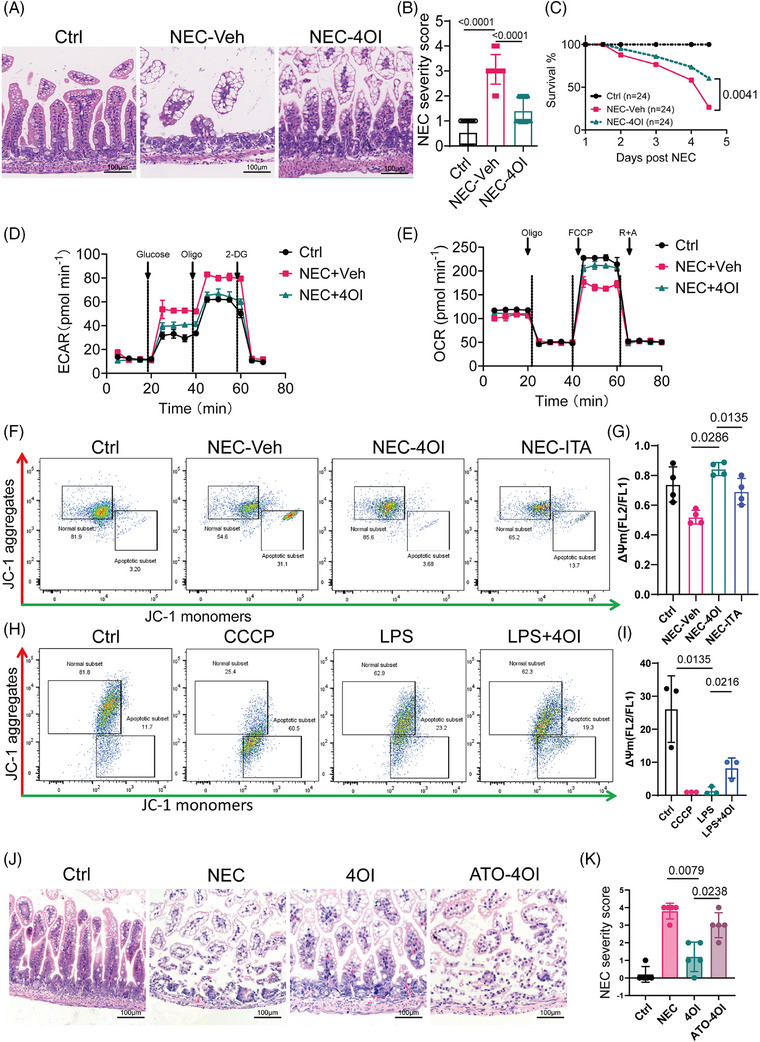
Background: Necrotizing enterocolitis (NEC) is a rapidly progressive and severe gastrointestinal disorder in neonates that is marked by an inflammatory cascade initiated by mechanisms that remain incompletely understood, resulting in intestinal necrosis and systemic infections. This study demonstrated that itaconate (ITA) exerts a protective effect in NEC by regulating macrophage reprogramming.
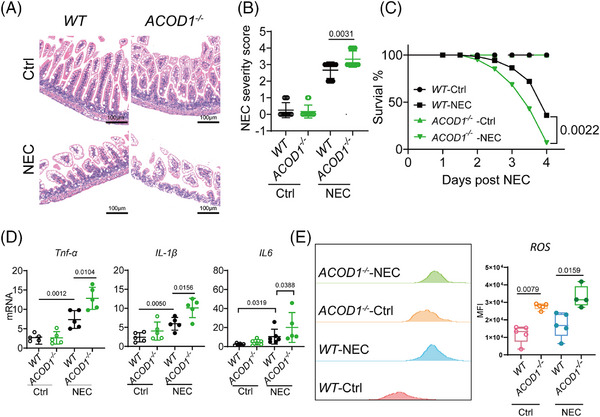
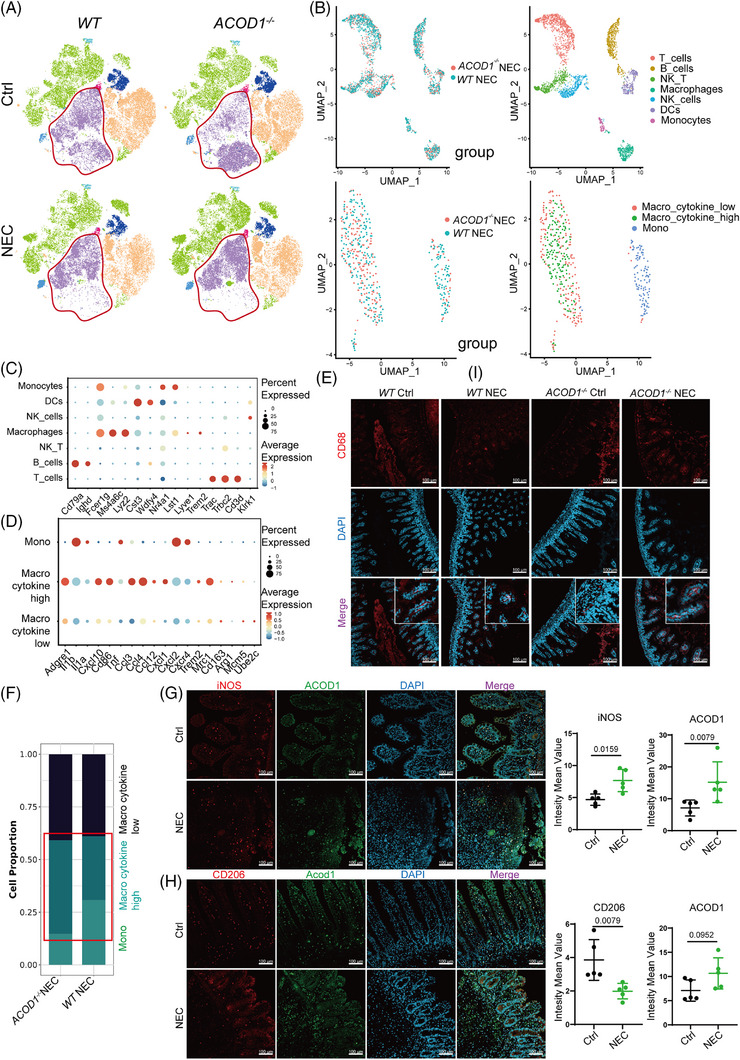
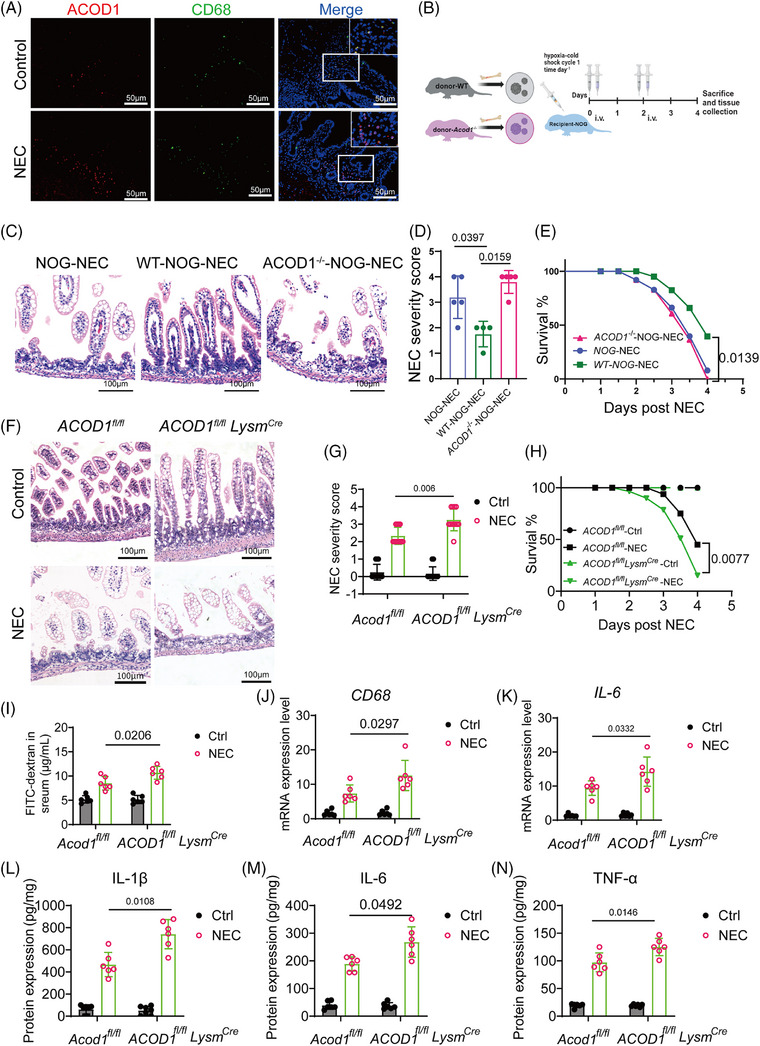
Methods: Changes in ITA expression were investigated using immunofluorescence staining and liquid chromatography-mass spectrometry, and their effect on immune cell differentiation was verified through single-cell sequencing. In vivo experiments were performed using ACOD1-/- and ACOD1fl/flLysMcre NEC mouse models.
Results: We detected changes in ITA expression in clinical NEC samples and confirmed the effect of these changes on immune cell differentiation. In vivo experiments confirmed the therapeutic role of ITA in regulating macrophage differentiation in NEC, and we further investigated the mechanism by which ITA regulates macrophage metabolic reprogramming. The depletion of ITA in NEC correlates with an increased frequency of pro-inflammatory macrophage polarization, thereby exacerbating intestinal inflammatory injury. Importantly, our in vivo experiments revealed that treatment with 4-octyl itaconate (4OI) significantly mitigated intestinal symptoms associated with NEC in murine models. Mechanistic investigations showed that 4OI effectively suppressed M1 macrophage polarization by rescuing mitochondrial function and upregulating oxidative phosphorylation in macrophages.
Conclusions: Our results highlight ITA as a metabolic checkpoint of macrophage differentiation in NEC and suggest the therapeutic efficacy of 4OI in NEC.
Key points: Itaconate alleviates NEC by reprogramming M1 macrophage metabolism ACOD1 deficiency exacerbates NEC severity 4OI maintains intestinal barrier integrity. 4OI rescues NEC by regulating macrophage mitochondrial activity.
Keywords: itaconate; macrophage; metabolic reprogramming; necrotizing enterocolitis; oxidative phosphorylation.
© 2025 The Author(s). Clinical and Translational Medicine published by John Wiley & Sons Australia, Ltd on behalf of Shanghai Institute of Clinical Bioinformatics.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Blakely ML, Tyson JE, Lally KP, et al. Initial Laparotomy versus peritoneal drainage in extremely low birthweight infants with surgical necrotizing enterocolitis or isolated intestinal perforation: a multicenter randomized clinical trial. Ann Surg. 2021;274(4):e370‐e380. doi: 10.1097/SLA.0000000000005099 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
- 82171695/National Natural Science Funds
- 82301955/National Natural Science Funds
- 82171709/National Natural Science Funds
- 82370526/National Natural Science Funds
- SL2024A03J01319/Science and Technology Program of Guangzhou
- SL2024A04J00240/Science and Technology Program of Guangzhou
- 2023BS015/Research Foundation of Guangzhou Women and Children's Medical Center for Clinical Doctor
- 2023M730791/the China Postdoctor Science Foundation
- 2024A1515013190/the Guangdong Basic and Applied Basic Research Foundation
- 2024A03J1238/Science and Technology Project of Guangzhou
- 2024A03J1171/Science and Technology Project of Guangzhou
- GJJ2203559/the Science and Technology Research Project of Education Department of Jiangxi Province
- 2024JXEYQM02/Jiangxi Provincial Children's Hospital 2024 First Batch "Qingmiao" Scientific Research Projects
- M1392/345 Talent Project of Shengjing Hospital
LinkOut - more resources
Full Text Sources