

Insights into absence of lymphoma despite fulminant Epstein-Barr virus infection in patients with XIAP deficiency
- PMID: 40674368
- PMCID: PMC12406724
- DOI: 10.1172/jci.insight.193787
Insights into absence of lymphoma despite fulminant Epstein-Barr virus infection in patients with XIAP deficiency
Abstract
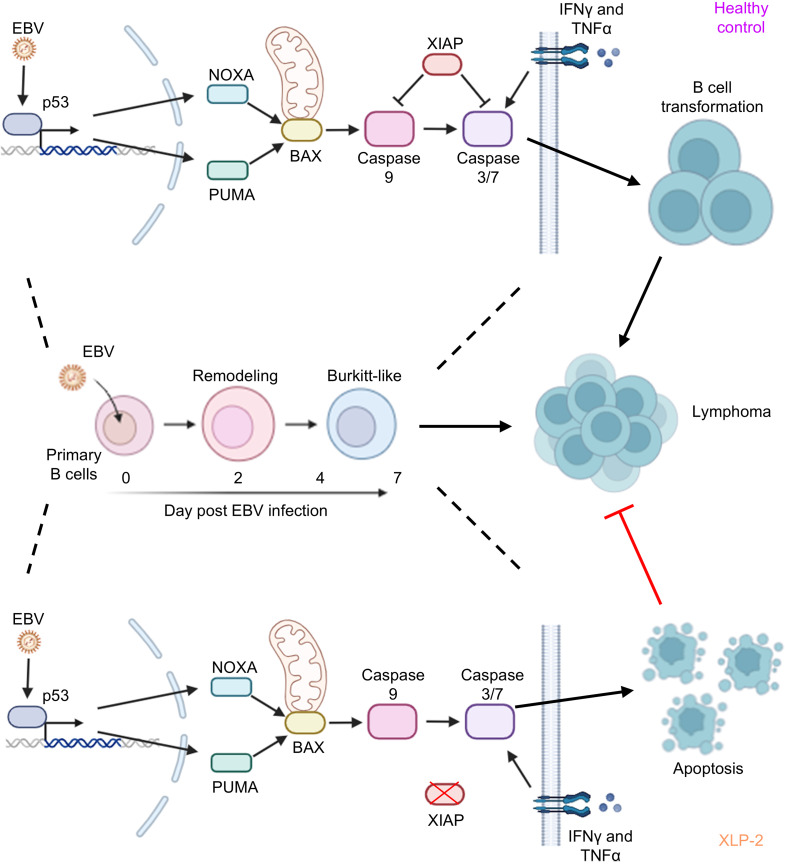
X-linked Lymphoproliferative Syndromes (XLP), arising from mutations in SH2D1A or XIAP genes, are characterized by fulminant Epstein-Barr virus (EBV) infection. Lymphomas occur frequently in XLP-1 and in other congenital conditions with heightened EBV susceptibility, but not in XLP-2. Why XLP-2 patients are apparently protected from EBV-driven lymphomagenesis remains a key open question. To gain insights, newly EBV-infected versus receptor-stimulated primary B cells from XLP-2 patients or with XIAP CRISPR editing were compared with healthy controls. XIAP perturbation impeded outgrowth of newly EBV-infected B cells, but not of CD40 ligand and interleukin-21-stimulated B cells. XLP-2-deficient B cells showed significantly lower EBV transformation efficiency than cells from healthy controls. Interestingly, EBV-immortalized lymphoblastoid cell proliferation was not impaired by XIAP knockout, implicating a XIAP role in early EBV B cell transformation. Mechanistically, nascent EBV infection activated p53-mediated apoptosis signaling, which was counteracted by XIAP in control cells. With XIAP deficiency, EBV markedly elevated apoptosis rates over the first 2 weeks of infection. IFN-γ, whose levels are increased with severe XLP2 EBV infection, markedly increased newly EBV-infected B cell apoptosis. These findings underscored XIAP's crucial role in support of the earliest stages of EBV-mediated B cell immortalization and provide insights into the curious absence of EBV+ lymphoma in patients with XLP-2.
Keywords: Apoptosis; Infectious disease; Lymphomas; Virology.
Conflict of interest statement
Figures





Update of
-
Insights into the Absence of Lymphoma Despite Fulminant Epstein-Barr Virus Infection in Patients with XIAP Deficiency.bioRxiv [Preprint]. 2025 Jan 18:2025.01.17.633616. doi: 10.1101/2025.01.17.633616. bioRxiv. 2025. Update in: JCI Insight. 2025 Jul 15;10(16):e193787. doi: 10.1172/jci.insight.193787. PMID: 39868266 Free PMC article. Updated. Preprint.
References
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
