

Identifying clusters of people with Multiple Long-Term Conditions using Large Language Models: a population-based study
- PMID: 40676244
- PMCID: PMC12271452
- DOI: 10.1038/s41746-025-01806-9
Identifying clusters of people with Multiple Long-Term Conditions using Large Language Models: a population-based study
Abstract
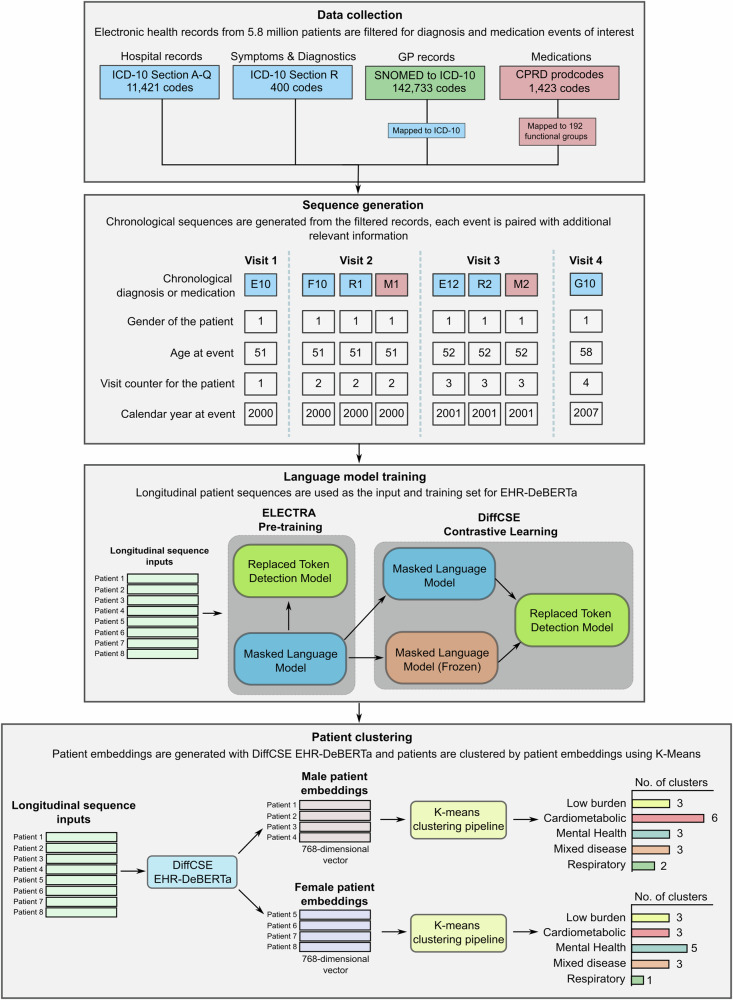
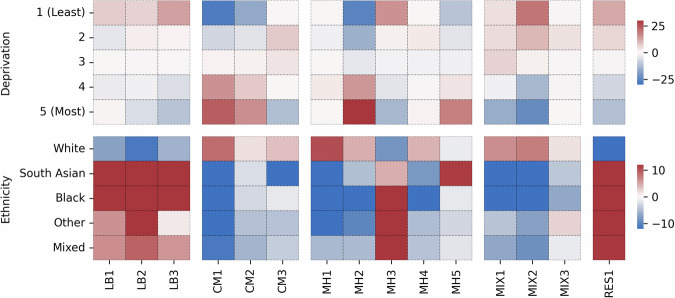
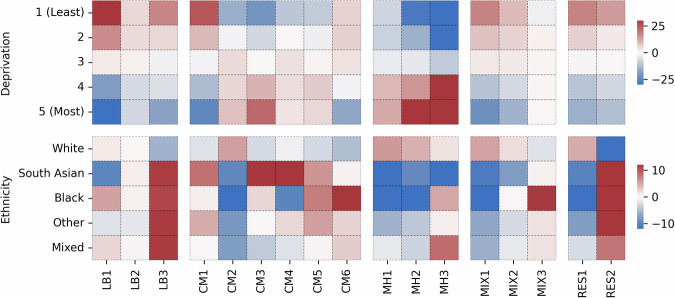
Identifying clusters of people with similar patterns of Multiple Long-Term Conditions (MLTC) could help healthcare services to tailor care. In this population-based study, we developed a pipeline incorporating a DeBERTa language model to generate gender-specific clusters. Our model, EHR-DeBERTa, was pre-trained on longitudinal sequences of diagnoses, medications and test results from primary care electronic health records of 5.8 million patients in the UK. EHR-DeBERTa was used to generate patient embeddings for males and females separately, and clusters were identified by K-Means. Fifteen clusters were identified in females and seventeen in males, categorized into low disease burden, mental health, cardiometabolic, respiratory and mixed diseases. Cardiometabolic and mental health conditions showed the strongest separation across clusters, with older patients in cardiometabolic clusters. Our approach demonstrates how LLMs can provide interpretable insights into disease patterns. Future work incorporating clinical outcomes could enhance risk prediction and support precision-medicine for people with MLTC.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures


References
-
- The Academy of Medical Sciences. Multimorbidity: A Priority for Global Health Research. https://acmedsci.ac.uk/file-download/82222577 (2018).
-
- Johnston, M. C., Crilly, M., Black, C., Prescott, G. J. & Mercer, S. W. Defining and measuring multimorbidity: a systematic review of systematic reviews. Eur. J. Public Health29, 182–189 (2019). - PubMed
-
- Pearson-Stuttard, J., Ezzati, M. & Gregg, E. W. Multimorbidity—a defining challenge for health systems. Lancet Public Health4, e599–e600 (2019). - PubMed
-
- Nunes, B. P., Flores, T. R., Mielke, G. I., Thumé, E. & Facchini, L. A. Multimorbidity and mortality in older adults: a systematic review and meta-analysis. Arch. Gerontol. Geriatr.67, 130–138 (2016). - PubMed
-
- Makovski, T. T., Schmitz, S., Zeegers, M. P., Stranges, S. & van den Akker, M. Multimorbidity and quality of life: systematic literature review and meta-analysis. Ageing Res. Rev.53, 100903 (2019). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
