

Decomposing socioeconomic and educational inequalities in infant mortality in Sub-Saharan Africa: DHS insights linked to countdown to 2030 and agenda 2063
- PMID: 40676638
- PMCID: PMC12273318
- DOI: 10.1186/s12889-025-23683-3
Decomposing socioeconomic and educational inequalities in infant mortality in Sub-Saharan Africa: DHS insights linked to countdown to 2030 and agenda 2063
Abstract
Introduction: Infant mortality, defined as the death of a baby within its first year of life, remains a critical public health issue, particularly in Sub-Saharan Africa (SSA). Health equity is a fundamental right, yet significant disparities persist, with poorer populations experiencing disproportionately higher mortality rates. This study aims to assess whether these inequalities in infant mortality continue despite governmental efforts and the pursuit of Sustainable Development Goals (SDGs) in SSA countries.
Methods: We analyzed a comprehensive dataset comprising 30,109 weighted samples from Demographic and Health Surveys across 14 SSA countries. Data cleaning was performed using Microsoft Excel, and statistical analyses were conducted with STATA Version 17 software. To evaluate wealth-related inequalities in infant mortality, we employed the concentration index and curve, alongside Wag staff decomposition analysis. A p-value of < 0.05 was considered statistically significant.
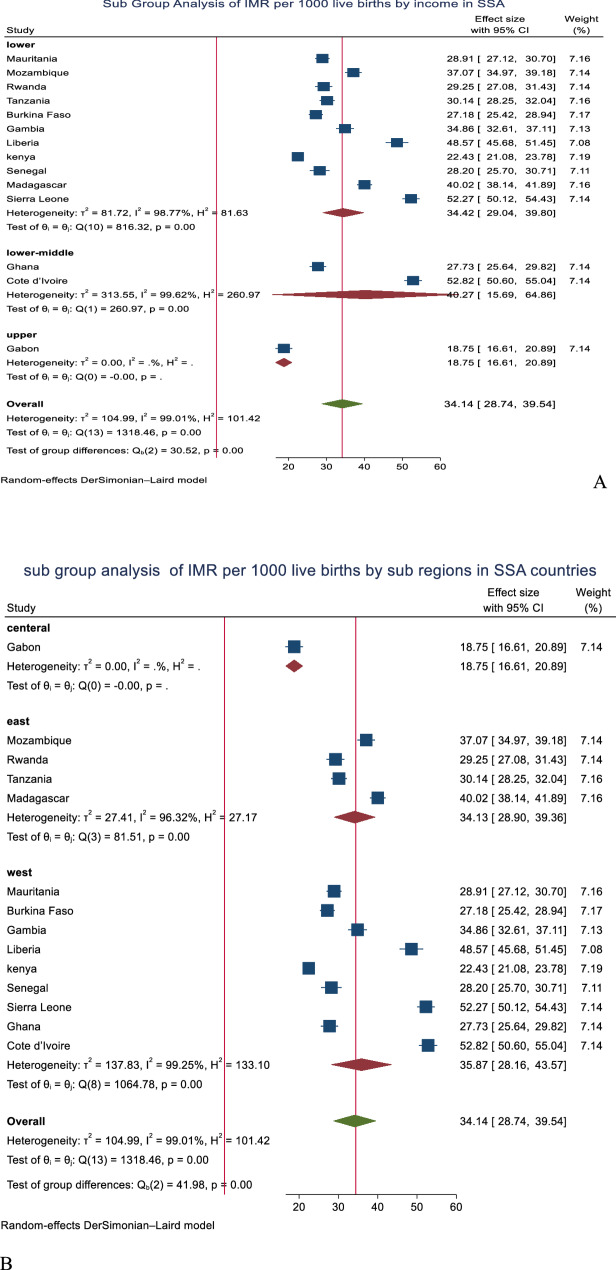
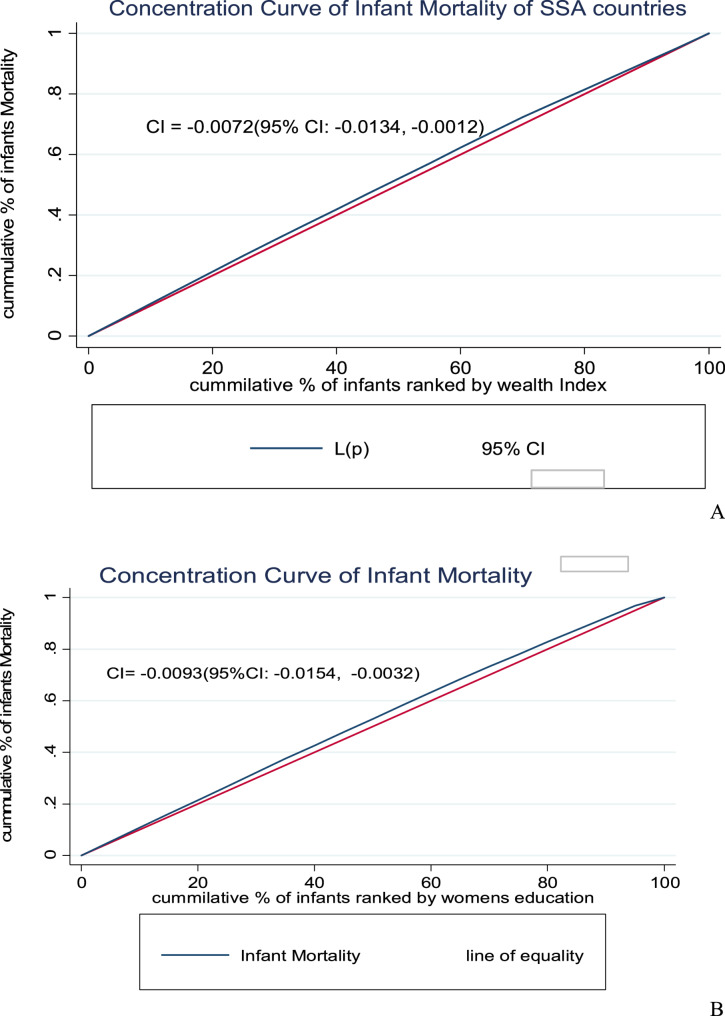
Result: The pooled estimate of the infant mortality rate in Sub-Saharan Africa was found to be 34.14% (95% CI: 28.74, 39.54%), with substantial heterogeneity (I² = 83.6%), indicates wide variation across the country. Rates varied significantly across countries, ranging from 18.75% in Gabon to 52.8% in Côte d'Ivoire. The weighted concentration index for infant mortality based on women's education was - 0.0072 (95% CI; -0.00134, -0.0012), while the wealth index concentration index was - 0.0093 (95% CI: -0.00154, -0.0032), both with p-values < 0.0001.
Conclusion and recommendation: Our analysis reveals that wealth-related disparities in infant mortality disproportionately impact poorer populations in Sub-Saharan Africa, with children of mothers who possess lower socioeconomic status and less education facing higher risks. Factors contributing to these disparities include family size, media exposure, and birth order. The persistence of social injustice is largely due to the inadequate response to these health inequalities. Policymakers must prioritize equitable access to healthcare and consider the socioeconomic distribution of infant mortality in their strategies. To combat these disparities and improve infant survival rates, it is vital to enhance child-rearing practices through targeted health policies, promote equitable economic development, engage communities in health initiatives, and establish monitoring systems. By focusing on these strategies, we can make significant progress toward reducing infant mortality and addressing the underlying social injustices affecting vulnerable populations in line with the goals of Countdown to 2030 and 2063.
Keywords: Infant mortality; Sub-Saharan Africa; Sustainable development goals; Wealth inequality.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethical approval and informed consent were not required for this specific study since it was a secondary data analysis of publicly available survey data from the measures DHS program. We requested DHS program data archivist, and permission be granted to download and use for this study from www.measuredhs.com . All the procedures were carried out in the relevant regulations and the declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Multilevel modelling of determinants of perinatal mortality in East Africa: a pooled analysis of National health survey data.BMC Public Health. 2025 May 30;25(1):2003. doi: 10.1186/s12889-025-23218-w. BMC Public Health. 2025. PMID: 40448089 Free PMC article.
-
Reducing health inequalities through general practice: a realist review and action framework.Health Soc Care Deliv Res. 2024 Mar;12(7):1-104. doi: 10.3310/YTWW7032. Health Soc Care Deliv Res. 2024. PMID: 38551093
-
Influence of paternal education on maternal and child health outcomes in Sub-Saharan Africa: evidence from demographic and health surveys.Reprod Health. 2025 Jul 29;22(1):137. doi: 10.1186/s12978-025-02086-y. Reprod Health. 2025. PMID: 40730994 Free PMC article.
-
Individual and community level determinants of unmeet pregnancy complication education among pregnant ANC visitor women in Sub-Saharan Africa: a multilevel analysis of the recent demographic and health survey.BMC Pregnancy Childbirth. 2025 Jul 9;25(1):733. doi: 10.1186/s12884-025-07843-2. BMC Pregnancy Childbirth. 2025. PMID: 40634865 Free PMC article.
-
Interventions targeted at women to encourage the uptake of cervical screening.Cochrane Database Syst Rev. 2021 Sep 6;9(9):CD002834. doi: 10.1002/14651858.CD002834.pub3. Cochrane Database Syst Rev. 2021. PMID: 34694000 Free PMC article.
References
-
- Ssewanyana S, Younger SD. Infant mortality in Uganda: Determinants, trends and the millennium development goals. J Afr Econ. 2008;17(1):34–61.
-
- Liu L, Hug L, Yeung D, You D. Newborn Mortality. InOxford Research Encyclopedia of Global Public Health. 2023.
-
- Organization WH. Children: reducing mortality. Wkly Epidemiol Record = Relevé Épidémiologique Hebdomadaire. 2014;89(38):418–20. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
