

Spontaneous ovulation, hormonal profiles, and the impact of progesterone timing variation on outcomes in natural proliferative phase frozen embryo transfer cycles with single euploid blastocyst transfer
- PMID: 40676677
- PMCID: PMC12273475
- DOI: 10.1186/s13048-025-01742-y
Spontaneous ovulation, hormonal profiles, and the impact of progesterone timing variation on outcomes in natural proliferative phase frozen embryo transfer cycles with single euploid blastocyst transfer
Abstract
Background: Natural cycle frozen embryo transfer (NC-FET) lowers obstetric risks by preserving ovulation and corpus luteum but limits scheduling flexibility. Natural proliferative phase FET (NPP-FET) offers a scheduling-friendly alternative, assuming ovulation is maintained after flexible progesterone (P4) initiation during the follicular phase. Only three peer-reviewed studies have investigated NPP-FET protocols, yet none verified spontaneous ovulation, characterized hormonal dynamics, or evaluated whether variation in P4 initiation timing influences clinical outcomes. Preserving spontaneous ovulation is essential for NPP-FET to replicate the physiologic benefits of NC-FET; confirming its consistency is critical to validating NPP-FET as a viable protocol. To our knowledge, this is the first study to comprehensively address these gaps, providing novel evidence to support NPP-FET's clinical feasibility.
Methods: This retrospective cohort study included 196 first-time NPP-FET cycles with single euploid blastocyst transfers between January 2023 and October 2024. Dydrogesterone (40 mg/day) was initiated upon meeting the following criteria: leading follicle ≥ 14 mm, endometrial thickness ≥ 7 mm, serum estradiol > 150 pg/mL, and P4 < 1.5 ng/mL. Ultrasound and hormonal monitoring continued until ultrasound-documented ovulation (UDO), followed by three days of hormone assessments. Ovulation was confirmed by UDO and serum P4 > 3.0 ng/mL. Embryo transfer occurred on day 6 of dydrogesterone exposure. Multivariable logistic regression evaluated associations between pregnancy outcomes and P4 timing-related variables, including follicular phase duration, estradiol and follicular diameter at P4 initiation, P4 start-to-UDO interval, UDO-to-FET interval, and serum P4 on FET day.
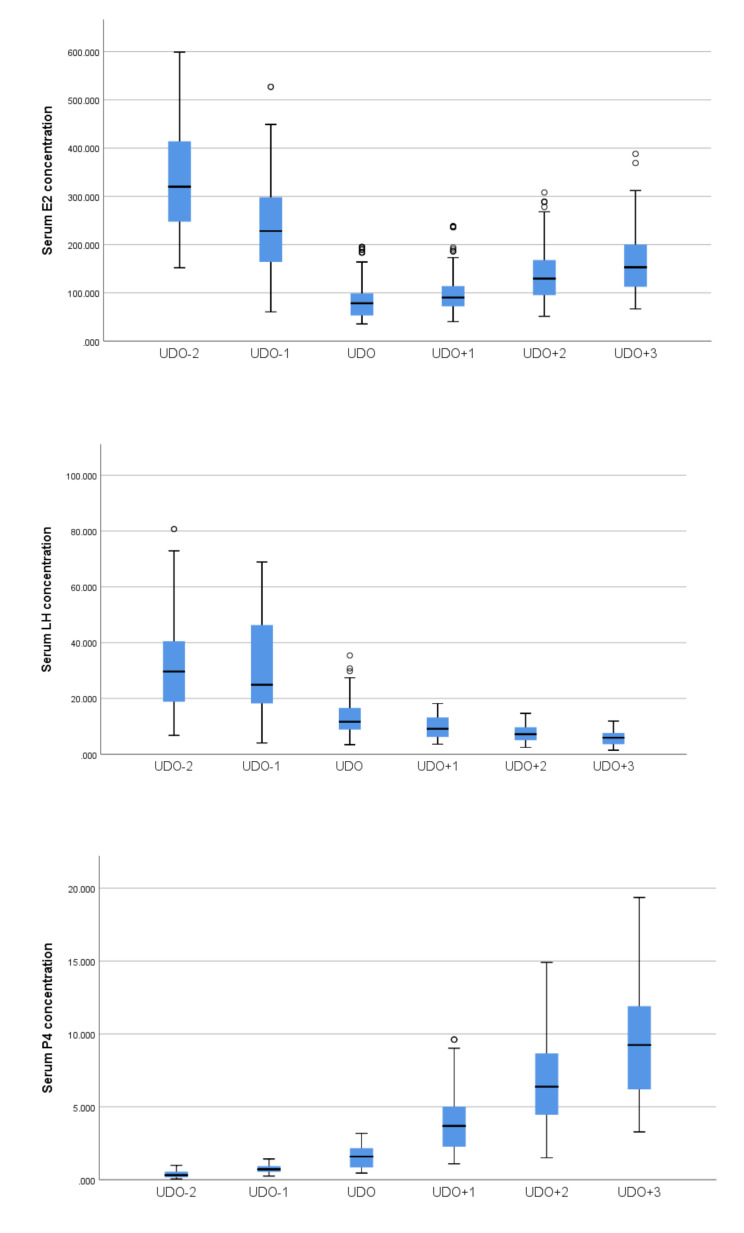
Results: Spontaneous ovulation was confirmed in all participants. Median follicular diameter one day before UDO was 18.6 mm. UDO occurred within 1-2 days in 96.4% and 92.2% of cases based on two LH surge criteria. Peri-ovulatory hormone profiles resembled natural cycles. Clinical pregnancy, ongoing pregnancy, and clinical loss rates were 66.3%, 58.7%, and 11.5%, respectively. Embryo morphology and biopsy day predicted pregnancy outcomes, while P4 timing-related variables showed no association.
Conclusions: Flexible dydrogesterone initiation at follicular diameters ≥ 14 mm, based on predefined criteria, preserves spontaneous ovulation and natural hormonal dynamics. Pregnancy outcomes were consistent across P4 initiation timings, supporting NPP-FET as a clinically viable, physiologically grounded, and scheduling-friendly protocol.
Keywords: Dydrogesterone; Endometrial Preparation; Euploid embryo; Frozen embryo transfer (FET); Modified natural cycle; Natural cycle; Natural proliferative phase frozen embryo transfer (NPP-FET); Spontaneous ovulation..
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: this retrospective study, approved by the institutional ethics committee review board of tri-service general hospital, national defense medical center, Taipei, Taiwan (C202405177), ensure that all research activities were conducted in accordance with the ethical standards and regulatory requirements. Consent for publication: not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Optimizing embryo transfer timing based on serum progesterone levels from a known implantation cohort: A retrospective observational study.J Formos Med Assoc. 2025 Aug 3:S0929-6646(25)00395-X. doi: 10.1016/j.jfma.2025.07.027. Online ahead of print. J Formos Med Assoc. 2025. PMID: 40759623
-
Cycle regimens for frozen-thawed embryo transfer.Cochrane Database Syst Rev. 2017 Jul 5;7(7):CD003414. doi: 10.1002/14651858.CD003414.pub3. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2025 Jun 3;6:CD003414. doi: 10.1002/14651858.CD003414.pub4. PMID: 28675921 Free PMC article. Updated.
-
Pregnancy and perinatal outcomes after modified natural cycle-frozen embryo transfers according to size of the dominant follicle on the hCG trigger day.Hum Reprod Open. 2025 Jul 16;2025(3):hoaf047. doi: 10.1093/hropen/hoaf047. eCollection 2025. Hum Reprod Open. 2025. PMID: 40799621 Free PMC article.
-
Estradiol and progesterone levels in early pregnancy after modified natural, programmed, and gonadotrophin-stimulated frozen embryo transfer cycles: a randomized controlled trial.Hum Reprod. 2025 Jul 1;40(7):1291-1304. doi: 10.1093/humrep/deaf083. Hum Reprod. 2025. PMID: 40389227 Clinical Trial.
-
Cycle regimens for endometrial preparation prior to frozen embryo transfer.Cochrane Database Syst Rev. 2025 Jun 3;6(6):CD003414. doi: 10.1002/14651858.CD003414.pub4. Cochrane Database Syst Rev. 2025. PMID: 40458990 Review.
References
-
- Roelens C, Blockeel C. Impact of different endometrial Preparation protocols before frozen embryo transfer on pregnancy outcomes: a review. Fertil Steril. 2022;118:820–7. - PubMed
-
- Lawrenz B, Blockeel C. Avoiding weekend frozen embryo transfer in modified natural cycles: is it possible? Reprod Biomed Online. 2024;49:103775. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
