

An 88-Year-Old Woman with a 33-Year History of Idiopathic Portal Hypertension Presenting with Hepatocellular Carcinoma Treated with Carbon-Ion Radiotherapy
- PMID: 40676829
- PMCID: PMC12282294
- DOI: 10.12659/AJCR.947725
An 88-Year-Old Woman with a 33-Year History of Idiopathic Portal Hypertension Presenting with Hepatocellular Carcinoma Treated with Carbon-Ion Radiotherapy
Abstract
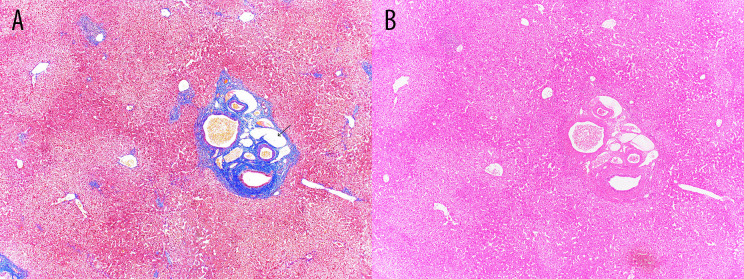
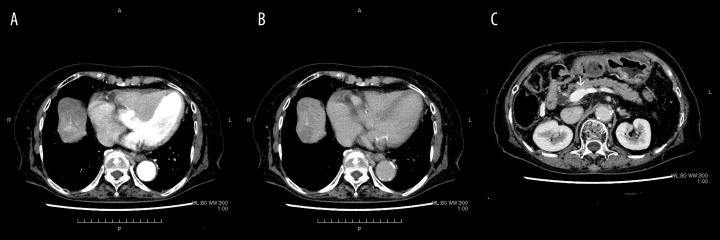
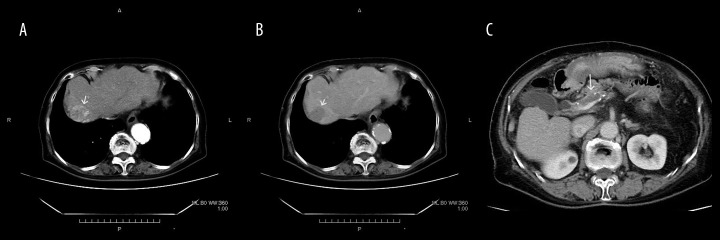
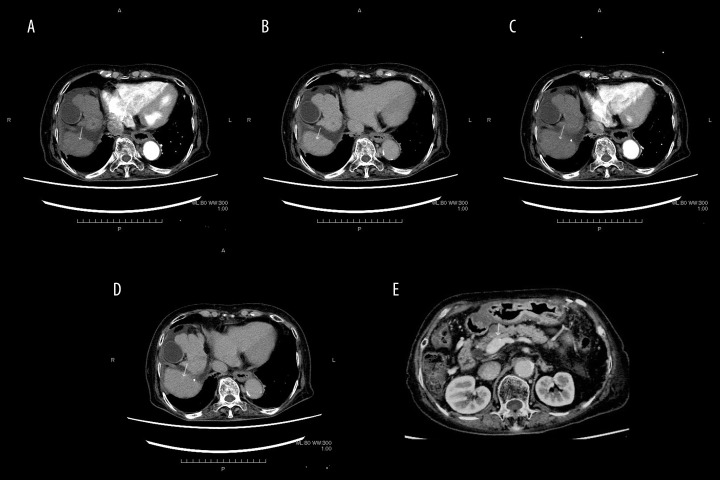
BACKGROUND Idiopathic portal hypertension (IPH) is a rare disease of unknown etiology that causes hypersplenism, splenomegaly, and portal hypertension. There have been rare reports of hepatocellular carcinoma (HCC) in patients with IPH, but no causal relationship has been confirmed. This report details the case of an 88-year-old Japanese woman who developed HCC after a 30-year history of IPH and was treated with carbon-ion radiotherapy. CASE REPORT An 88-year-old Japanese woman had presented to our hospital 33 years earlier with bleeding from esophageal varices. Liver function test results were normal. Computed tomography (CT) showed marked splenomegaly. She had no known causative factors for liver disease, and IPH was suspected. Endoscopic injection sclerotherapy was performed repeatedly for episodes of bleeding from esophageal varices until 4 years after presentation, when she underwent Hassab's procedure. A liver biopsy showed preserved lobular architecture and moderate fibrous enlargement of the portal area without necro-inflammatory reaction. She had a stroke 18 years later and was started on clopidogrel. Nine years later, CT revealed a 24-mm HCC in S8, and portal vein thrombosis (PVT). Carbon-ion radiotherapy was administered, followed by edoxaban. Three months later, CT showed shrinkage of the HCC and complete resolution of the PVT. Almost 3 years later, CT showed no recurrence of HCC or PVT. CONCLUSIONS We report a rare case of IPH and HCC co-existing in a patient followed up for more than 30 years. Although there is no recognized association between IPH and HCC, this report highlights the importance of continued clinical follow-up of patients with chronic liver disease.
Conflict of interest statement
Figures
Similar articles
-
Platelet count, spleen length, and platelet count-to-spleen length ratio for the diagnosis of oesophageal varices in people with chronic liver disease or portal vein thrombosis.Cochrane Database Syst Rev. 2017 Apr 26;4(4):CD008759. doi: 10.1002/14651858.CD008759.pub2. Cochrane Database Syst Rev. 2017. PMID: 28444987 Free PMC article.
-
Endoscopic injection of cyanoacrylate glue versus other endoscopic procedures for acute bleeding gastric varices in people with portal hypertension.Cochrane Database Syst Rev. 2015 May 12;2015(5):CD010180. doi: 10.1002/14651858.CD010180.pub2. Cochrane Database Syst Rev. 2015. PMID: 25966446 Free PMC article.
-
Ablative and non-surgical therapies for early and very early hepatocellular carcinoma: a systematic review and network meta-analysis.Health Technol Assess. 2023 Dec;27(29):1-172. doi: 10.3310/GK5221. Health Technol Assess. 2023. PMID: 38149643 Free PMC article.
-
Management of people with early- or very early-stage hepatocellular carcinoma: an attempted network meta-analysis.Cochrane Database Syst Rev. 2017 Mar 28;3(3):CD011650. doi: 10.1002/14651858.CD011650.pub2. Cochrane Database Syst Rev. 2017. PMID: 28351116 Free PMC article.
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
