

A Multinational Cohort Study of Dialysis Initiation During Pregnancy
- PMID: 40677311
- PMCID: PMC12266275
- DOI: 10.1016/j.ekir.2025.03.057
A Multinational Cohort Study of Dialysis Initiation During Pregnancy
Abstract
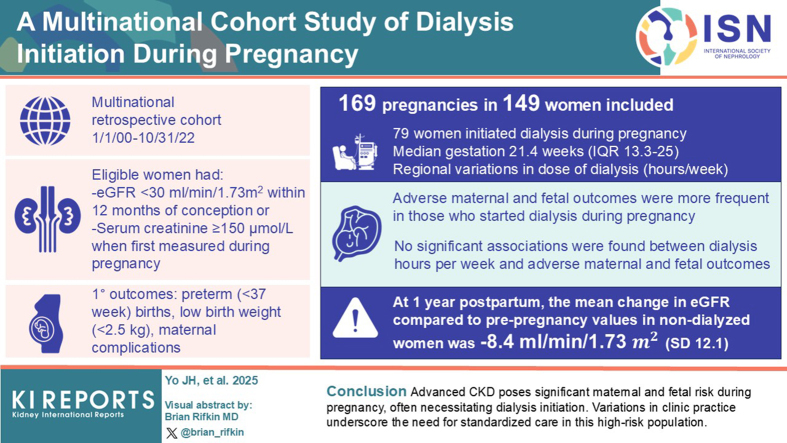
Introduction: There are insufficient data to guide the initiation of dialysis in pregnancy, contributing to wide variation in practice and uncertainty in the management of this high-risk population. Our study aimed to examine dialysis initiation patterns in pregnancy, describe adverse pregnancy outcomes in women with advanced chronic kidney disease (CKD), and assess the impact of dialysis hours on these outcomes.
Methods: We conducted a multinational retrospective cohort study of women who delivered between January 1, 2000 and October 31, 2022. Eligible women had either a prepregnancy estimated glomerular filtration rate (eGFR) <30 ml/min per 1.73 m2 within 12 months of conception, or a serum creatinine ≥ 150 μmol/l when first measured during pregnancy. For pregnancies where dialysis was initiated, regional differences in dialysis indications, prescriptions, and laboratory data were described. Adverse maternal and fetal outcomes were assessed for all pregnancies.
Results: A total of 169 pregnancies in 149 women were included; 79 (46.7%) initiated dialysis during pregnancy at a median of 21.4 weeks' gestation (interquartile range [IQR]: 13.3-25.0). There were regional differences in dialysis initiation and dose (hours/wk). Adverse maternal and fetal outcomes were more frequent in women who started dialysis during pregnancy. No significant associations were observed between dialysis hours/wk and adverse maternal and fetal outcomes. At 1 year postpartum, the mean change in eGFR compared with prepregnancy values in nondialyzed women was -8.4 ml/min per 1.73 m2 (SD: 12.1).
Conclusion: Advanced CKD poses significant maternal and fetal risks during pregnancy, often necessitating dialysis initiation. Variations in clinical practice underscore the need for standardized care in this high-risk population.
Keywords: dialysis; end-stage kidney disease; obstetric nephrology; pregnancy.
© 2025 Published by Elsevier, Inc., on behalf of the International Society of Nephrology.
Figures

References
-
- Mackay E.V. Pregnancy and renal disease: a ten-year survey. Aust N Z J Obstet Gynaecol. 1963;3:21–34. doi: 10.1111/j.1479-828X.1963.tb00210.x. - DOI
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
