

Comparison of the magnetic resonance elastography and FIB-4 (MEFIB) Index and vibration-controlled transient elastography for significant metabolic dysfunction-associated steatotic liver disease fibrosis
- PMID: 40677533
- PMCID: PMC12269210
- DOI: 10.3138/canlivj-2024-0007
Comparison of the magnetic resonance elastography and FIB-4 (MEFIB) Index and vibration-controlled transient elastography for significant metabolic dysfunction-associated steatotic liver disease fibrosis
Abstract
Background: Significant fibrosis (≥stage 2) in patients with metabolic dysfunction-associated steatotic liver disease (MASLD) is considered a high risk for morbidity and mortality. The magnetic resonance elastography (MRE) and FIB-4 (MEFIB) Index (MRE ≥ 3.3 kPa and FIB-4 ≥ 1.6) has been proposed as an alternative to liver biopsy, particularly in identifying patients for therapeutic intervention. However, MRE is not widely available. Our aim was to compare the MEFIB Index with other simpler, non-invasive markers.
Methods: A single-centre retrospective analysis of steatotic liver disease patients with MRE and vibration-controlled transient elastography (VCTE) was carried out between March 2019 and June 2022. Demographic and laboratory data were collected to calculate various fibrosis scores.
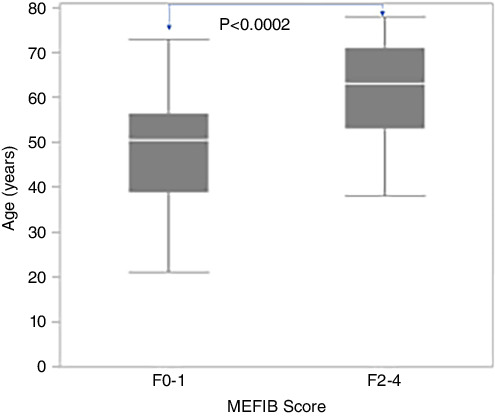
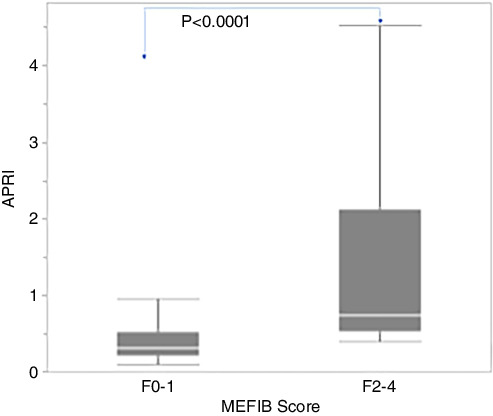
Results: Our cohort included 77 patients with a mean ± SD age of 51 ± 13 years, 44/77 (57%) female, BMI 34.5 ± 6.7 kg/m2, and 33/77 (43%) with diabetes mellitus. Significant MEFIB Index fibrosis (F2-4) compared with F0-1 was significantly associated with older age (61.6 versus 48.9 years), higher VCTE score (18.2 versus 10.6 kPa), NAFLD Fibrosis Score (0.11 versus -1.68), and Aspartate Aminotransferase-To-Platelet Ratio Index (APRI; 1.43 versus 0.44). A logistic regression model showed that age (odds ratio [OR]: 1.16; 95% CI: 1.05-1.29; p = 0.005) and APRI (OR: 10.86; 95% CI: 1.56-75.68; p = 0.016) were independently associated with MEFIB Index and predicted MEFIB F ≥ 2 with an area under the receiver operating characteristic curve of 0.95 (95% CI: 0.87-0.98).
Conclusions: In patients with MASLD, simple clinical and biochemical parameters may provide an alternative to predict significant fibrosis based on the MEFIB score. This may be useful in non-tertiary centres where VCTE and MRE are not routinely available.
Keywords: MR elastography; fatty liver; liver fibrosis; non-invasive test; steatosis; transient elastography.
Plain language summary
Lay Summary: Metabolic dysfunction–associated steatotic liver disease (MASLD), earlier known as non-alcoholic fatty liver disease, is a growing global health concern that is becoming more prevalent. There has always been a search for an accurate non-invasive imaging or blood test to identify patients with metabolic dysfunction–associated steatohepatitis (MASH) and advanced fibrosis. There has been a constant effort to develop a combination of serum- and imaging-based tests to diagnose fibrosis stages without the need for a liver biopsy. Unfortunately, magnetic resonance (MR) elastography (MRE) is not readily accessible and comes at a high cost. In this study, we validated simple clinical and laboratory parameters to predict MRE and FIB-4 Index (MEFIB) scores in our MASLD cohort. We developed a simple test that incorporates age and the Aspartate Aminotransferase-To-Platelet Ratio Index (APRI), which can diagnose advanced fibrosis at an accuracy of over 80%. In conclusion, this study provides a simple alternative to diagnose advanced MASH fibrosis based on the MEFIB index.
© Canadian Association for the Study of the Liver, 2024.
Conflict of interest statement
N/A
Figures
References
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous