

Prevention and treatment of recurrence after endoscopic resection of large non-pedunculated colorectal polyps
- PMID: 40677574
- PMCID: PMC12264792
- DOI: 10.4253/wjge.v17.i7.107746
Prevention and treatment of recurrence after endoscopic resection of large non-pedunculated colorectal polyps
Abstract
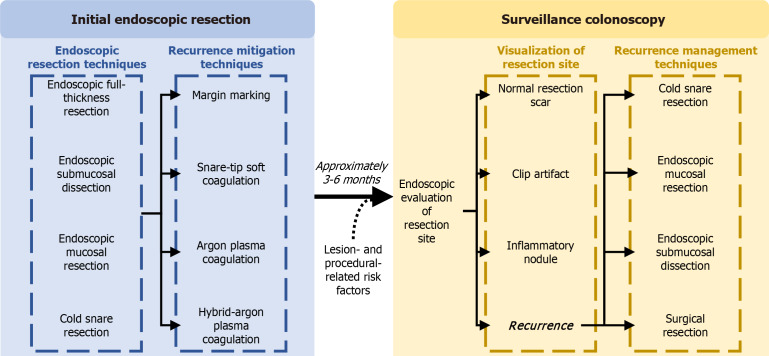
Minimally invasive endoscopic resection techniques are the recommended first-line treatment strategy for the majority of large non-pedunculated colorectal polyps, with endoscopic mucosal resection (EMR) as a predominant resection modality due to its efficacy, efficiency, safety, and cost-effectiveness. A limitation of EMR is recurrence, which has historically occurred in 15%-20% of lesions. In the past 10 years, a number of effective mitigating strategies have been developed, including margin thermal ablation using snare-tip soft coagulation, argon plasma coagulation (APC), and hybrid-APC, alongside margin marking pre-resection. Moreover, techniques for effective recurrence management have also been developed. Herein, we appraise existing evidence on the frequency of recurrence, reasonings behind recurrence formation, as well as recurrence mitigating strategies and the effectiveness of recurrence management.
Keywords: Adenoma; Cancer; Colonoscopy; Endoscopy; Polyp.
©The Author(s) 2025. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: Shahidi N received a speaker’s honorarium from Pharmascience, Boston Scientific, and Takeda Pharmaceuticals. Pang S and Tavakoli P have no conflict of interests to report.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
