

Comparative study of brain activity and functional connectivity in blepharospasm and blepharospasm-oromandibular dystonia
- PMID: 40677687
- PMCID: PMC12268265
- DOI: 10.3389/fneur.2025.1583297
Comparative study of brain activity and functional connectivity in blepharospasm and blepharospasm-oromandibular dystonia
Abstract
Background: The most common spread of blepharospasm (BSP) is to the oromandibular region, labeled as blepharospasm-oromandibular dystonia (BOM). We aimed to identify shared and different functional changes in BSP and BOM, trying to unveil the pathogenesis of these disorders and the mechanism of dystonic spread.
Materials and methods: This single center study recruited 16 BSP patients, 16 BOM patients and 20 healthy controls (HC). Clinical information and resting-state fMRI images were collected. Dynamic amplitude of low-frequency fluctuations (dALFF) was calculated using the sliding window method. Intergroup differences in static ALFF (sALFF) and dALFF were examined. Using dALFF results, seed-based static and dynamic functional connectivity (FC) were constructed to compare connectivity changes in BSP and BOM networks. Correlations between dynamic parameters and disease severity scores were analyzed using Spearman partial correlation.
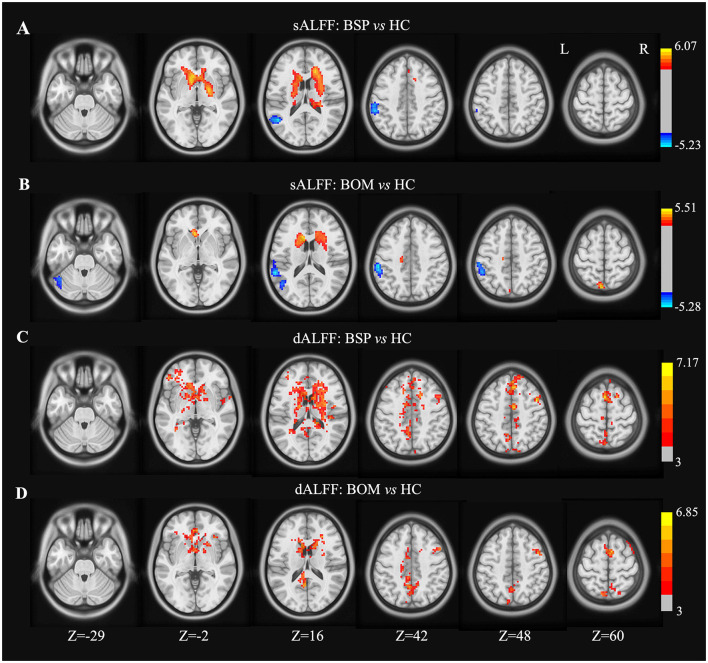
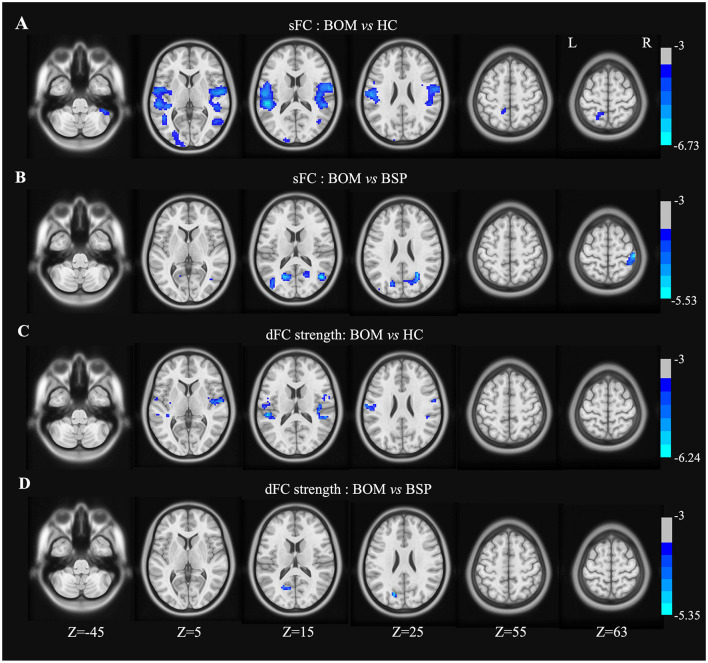
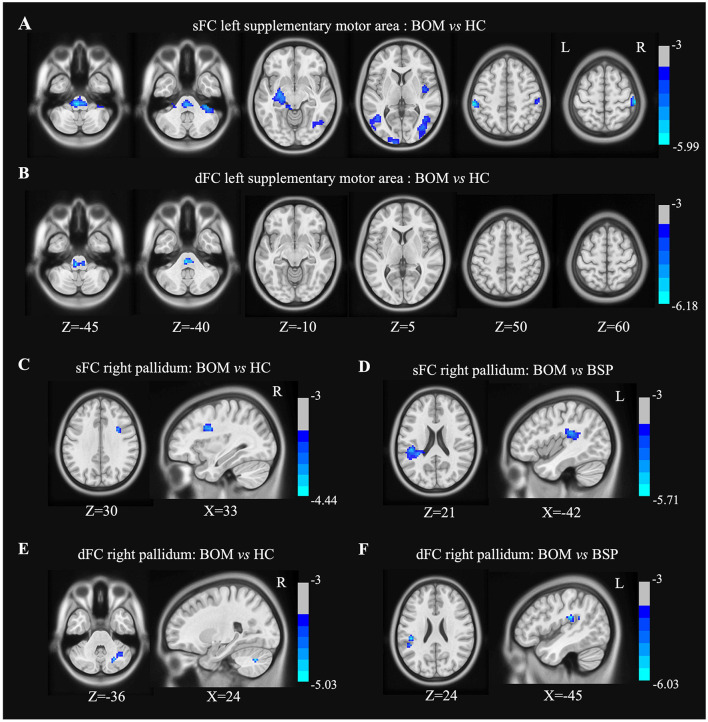
Results: Compared with HC, BSP and BOM presented increased dALFF in the bilateral basal ganglia, bilateral supplementary motor area, right precentral gyrus, and bilateral cingulate gyrus. BOM further demonstrated decreased sALFF in the left cerebellum. Compared with HC, BOM patients had decreased sFC in the network involving the sensorimotor cortex, supplementary motor area, basal ganglia, cerebellum, and brainstem. In addition, decreased dFC strength was found between the right pallidum and cerebellum. Comparing with BSP patients, BOM patients showed decreased sFC and dFC strength in a similar but limited pattern. Clinical scores of BSP severity were significantly correlated with dALFF in some of these important regions.
Conclusions: Our results demonstrated common brain regions with impaired functional activity in BSP and BOM patients. Further, BOM is featured with widespread connectivity reduction in the sensorimotor cortico-basal ganglia-brainstem-cerebellar network deriving from these key regions. These findings could help investigate mechanisms of dystonia spread and potentially facilitate disease-modifying therapies.
Keywords: blepharospasm; blepharospasm-oromandibular dystonia; dynamic ALFF; dynamic FC; fMRI.
Copyright © 2025 Wang, Luo, Hou, Li, Yang, Feng, Wang and Wan.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Increased functional connectivity coupling with supplementary motor area in blepharospasm at rest.Brain Res. 2023 Oct 15;1817:148469. doi: 10.1016/j.brainres.2023.148469. Epub 2023 Jun 22. Brain Res. 2023. PMID: 37355150
-
Abnormal dynamic brain activity and functional connectivity of primary motor cortex in blepharospasm.Eur J Neurol. 2022 Apr;29(4):1035-1043. doi: 10.1111/ene.15233. Epub 2022 Jan 6. Eur J Neurol. 2022. PMID: 34962021
-
Brain functional alterations in early stage of coal workers' pneumoconiosis with alcoholism: insights from a resting-state fMRI investigation.Front Neurosci. 2025 Jun 16;19:1610657. doi: 10.3389/fnins.2025.1610657. eCollection 2025. Front Neurosci. 2025. PMID: 40589788 Free PMC article.
-
Altered brain connectivity in hyperkinetic movement disorders: A review of resting-state fMRI.Neuroimage Clin. 2023;37:103302. doi: 10.1016/j.nicl.2022.103302. Epub 2022 Dec 24. Neuroimage Clin. 2023. PMID: 36669351 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
References
LinkOut - more resources
Full Text Sources