

Optimizing pediatric "Mild" traumatic brain injury assessments: A multi-domain random forest analysis of diagnosis and outcomes
- PMID: 40678189
- PMCID: PMC12269848
- DOI: 10.1016/j.ijchp.2025.100600
Optimizing pediatric "Mild" traumatic brain injury assessments: A multi-domain random forest analysis of diagnosis and outcomes
Abstract
Objective: Despite advances in imaging and fluid-based biomarkers, the care for pediatric "mild" traumatic brain injury (pmTBI) remains primarily dependent on clinical evaluation. However, the optimal clinical assessments for diagnosing pmTBI and predicting outcomes remain debated, including which individual test or combinations of assessments are most effective, and how this evolves as a function of time post-injury.
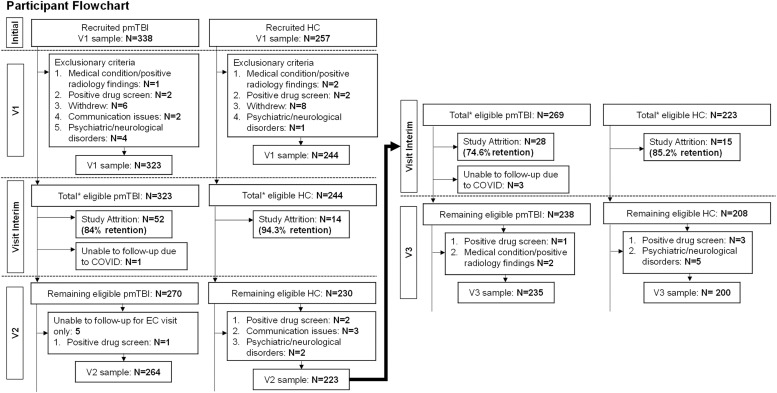
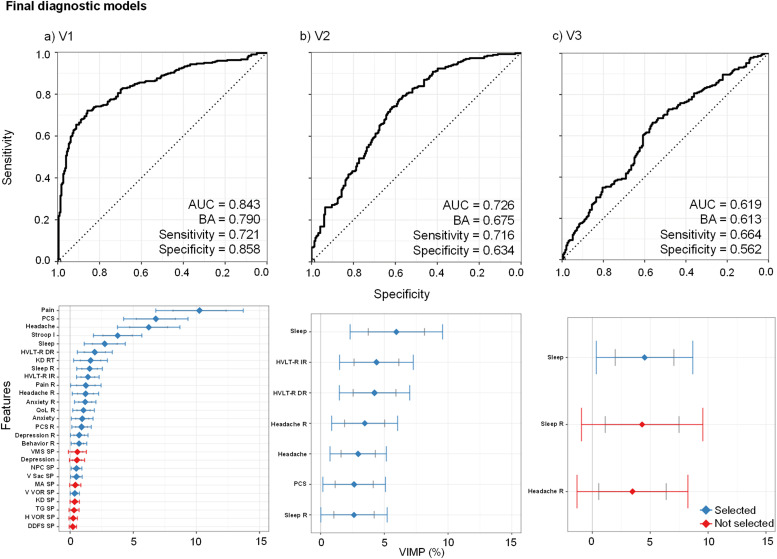
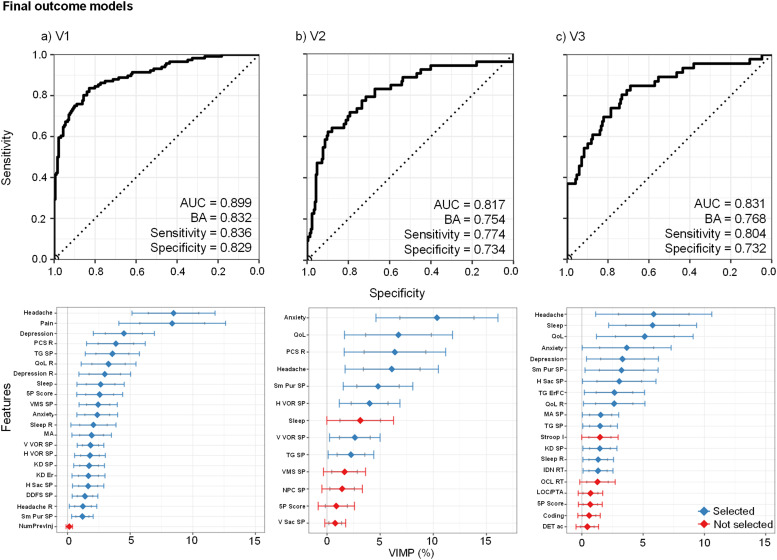
Method: Random Forest models were used to identify the most effective assessments for diagnostic (pmTBI vs. healthy controls) and outcome (pmTBI with favorable vs. poor outcomes, based on persisting symptoms) classification accuracy across a comprehensive battery including domains of self-reported clinical-ratings, paper-and-pencil cognitive tests, computerized cognitive tests, symptom provocation during neurosensory tests, and performance-based neurosensory measures. Assessments were conducted within 11-days, at 4-months and 1-year post-injury to examine acute and long-term recovery trajectories. A total of 323 pmTBI (180 males; age 14.5 ± 2.8 years) and 244 HC (134 males, 14.0 ± 2.9 years) were included (∼75 % 1-year retention) in final analyses.
Results: Self-reported clinical-ratings outperformed performance-based metrics across all visits in both models, with somatic complaints demonstrating the highest predictive validity. Cognitive tests of memory aided diagnostic classification, while emotional disturbances were predictive of outcome classification up-to 4-months. Retrospective ratings, reflecting trait-like characteristics, were more predictive for identifying individuals at risk of poor outcomes. Computerized cognitive and neurosensory tests had limited predictive value beyond 1-week post-injury.
Conclusions: Clinicians should adopt a tailored approach for clinical assessments across different post-injury intervals to enhance clinical care, shorten assessment batteries, and better understand recovery in children with "mild" TBI.
Keywords: Clinical assessments; Diagnostic classification; Machine learning; Mild traumatic brain injury; Outcome classification; Pediatric.
© 2025 The Authors. Published by Elsevier B.V.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Andrew R. Mayer reports financial support was provided by National Institutes of Health. If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Clinical symptoms, signs and tests for identification of impending and current water-loss dehydration in older people.Cochrane Database Syst Rev. 2015 Apr 30;2015(4):CD009647. doi: 10.1002/14651858.CD009647.pub2. Cochrane Database Syst Rev. 2015. PMID: 25924806 Free PMC article.
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
References
-
- Babikian T., Satz P., Zaucha K., Light R., Lewis R.S., Asarnow R.F. The UCLA longitudinal study of neurocognitive outcomes following mild pediatric traumatic brain injury. Journal of the International Neuropsychological Society : JINS. 2011;17(5):886–895. doi: 10.1017/S1355617711000907. - DOI - PMC - PubMed
-
- Beauchamp M.H., Aglipay M., Yeates K.O., Desire N., Keightley M., Anderson P.…Zemek R. Predictors of neuropsychological outcome after pediatric concussion. Neuropsychology. 2018;32(4):495–508. [2018-24118-008 pii;10.1037/neu0000419] PM:29809036. - PubMed
-
- Breiman L. Random forests. Machine learning. 2001;45(1):5–32.
LinkOut - more resources
Full Text Sources
