

This is a preprint.
Identification of Chlamydia pneumoniae and NLRP3 inflammasome activation in Alzheimer's disease retina
- PMID: 40678205
- PMCID: PMC12270195
- DOI: 10.21203/rs.3.rs-6658954/v1
Identification of Chlamydia pneumoniae and NLRP3 inflammasome activation in Alzheimer's disease retina
Update in
-
Identification of Chlamydia pneumoniae and NLRP3 inflammasome activation in Alzheimer's disease retina.Nat Commun. 2026 Jan 22;17(1):771. doi: 10.1038/s41467-026-68580-4. Nat Commun. 2026. PMID: 41571675 Free PMC article.
Abstract
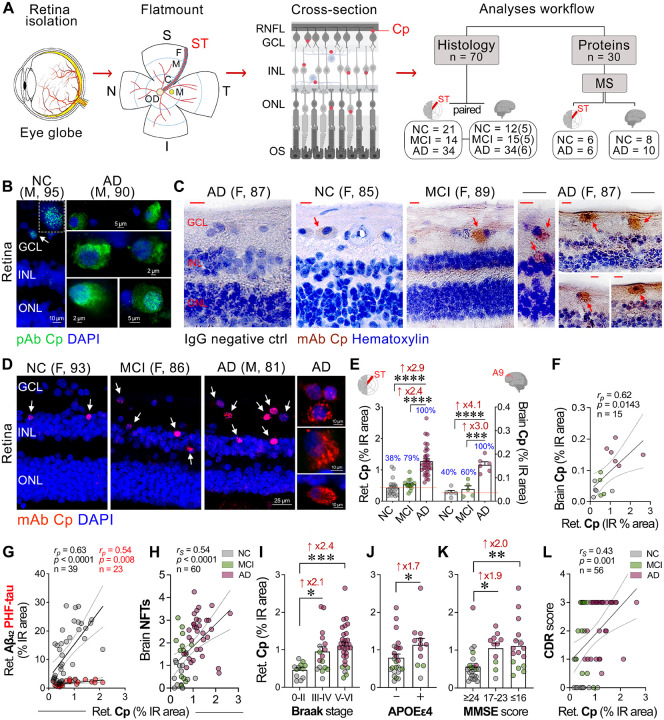
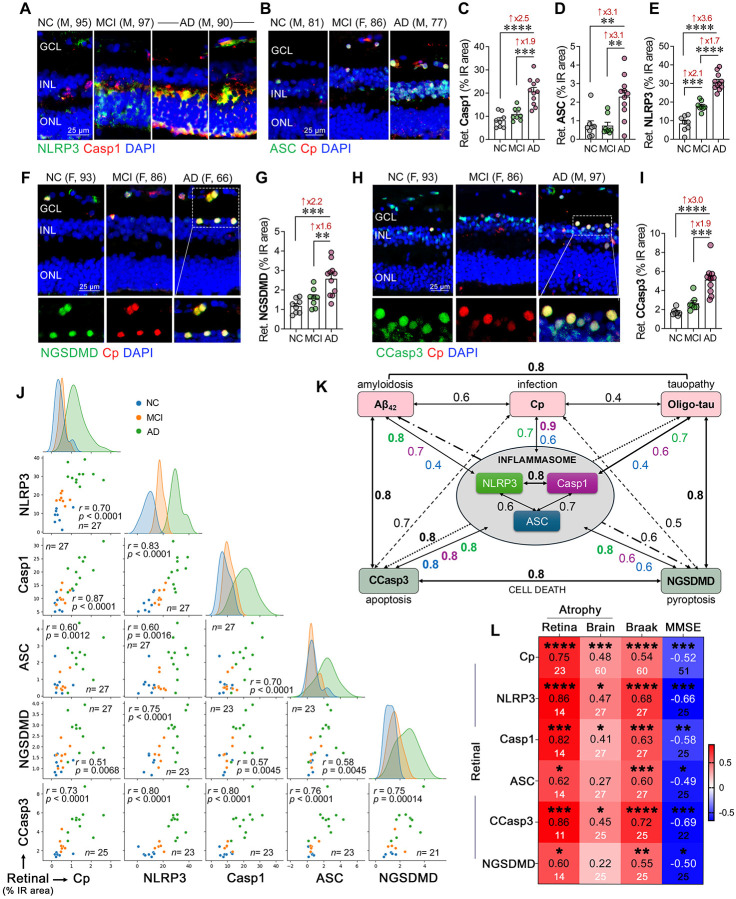
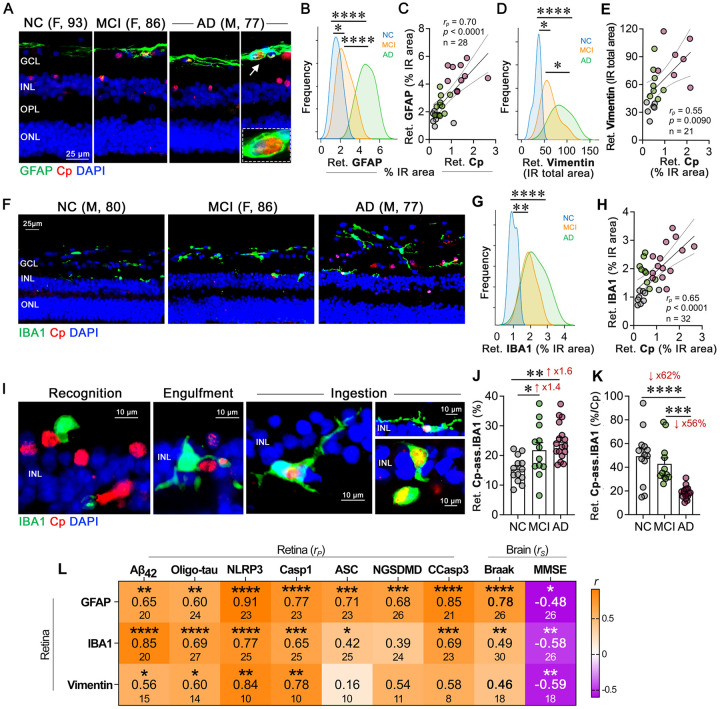
Emerging evidence implicates bacterial infections, including Chlamydia pneumoniae (Cp), a gram-negative obligate intracellular bacterium responsible for community-acquired pneumonia, in Alzheimer's disease (AD) pathogenesis. However, the involvement of Cp in early and advanced AD in the retina is unknown. Here, we identified the existence and distribution of intracellular Cp inclusions and related NLRP3 inflammasome activation and neurodegeneration in postmortem retinas and brains from 95 human donors. Histological analysis in neuropathologically-confirmed MCI and AD patients compared with cognitively normal individuals (n=70), revealed 2.9-4.1-fold increases of Cp inclusions in AD retinas and brains, respectively, with no significant increases in MCI retinas or brains. Mass spectrometry-based proteomics in additional cohorts (n=30), revealed dysregulated brain and retinal bacterial infection-related proteins and inflammasome-associated pathways. Retinal Cp was strongly linked to Aβ42, caspase-1 and NLRP3-inflammasome activation components, as well as cleaved caspase-3+ apoptosis and cleaved gasdermin D pyroptotic cell death. Despite increased IBA1+ microgliosis in the AD retina, the Cp-associated microglial population was reduced by 62%, suggesting impaired microglial phagocytosis. Higher retinal Cp burden correlated with APOEε4 status, advanced Braak stage, and cognitive decline. Machine learning models revealed that retinal Cp or NLRP3, in combination with retinal Aβ42, effectively predicted AD diagnosis, Braak stage, and cognition. These findings suggest that Cp infection contributes to AD dementia but is unlikely to initiate AD pathological changes, whereas elevated retinal NLRP3 may serve as an early AD marker. These results underscore the need for future studies investigating Cp's role in AD dementia and testing early antibiotic or inflammasome-targeting therapies.
Keywords: Alzheimer’s disease; Chlamydia pneumoniae (Cp); NLRP3 inflammasome; apoptosis; gliosis; machine learning; retina.
Conflict of interest statement
Conflict of interest All other authors declare no conflict of interest related to this work. Unrelated to this study: YK, KLB, and MKH are co-founding members in NeuroVision Imaging, Inc., Sacramento, CA, USA. Additional Declarations: There is NO Competing Interest.
Figures


References
-
- The top 10 causes of death. World Health Organization. 2024;
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
