

Global burden of chronic kidney disease and its attributable risk factors (1990-2021): an analysis based on the global burden of disease study
- PMID: 40678313
- PMCID: PMC12267038
- DOI: 10.3389/fendo.2025.1563246
Global burden of chronic kidney disease and its attributable risk factors (1990-2021): an analysis based on the global burden of disease study
Abstract
Background: Chronic kidney disease is a global health challenge, especially in resource-limited regions. Understanding its burden and key risk factors is crucial for effective interventions.
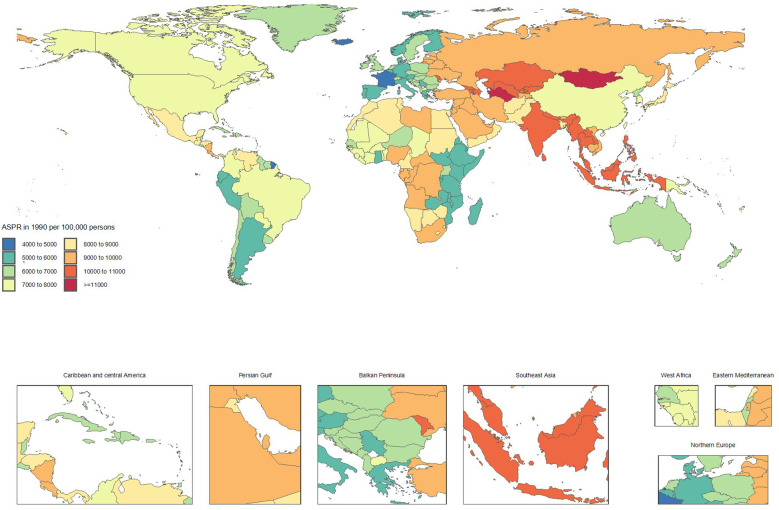
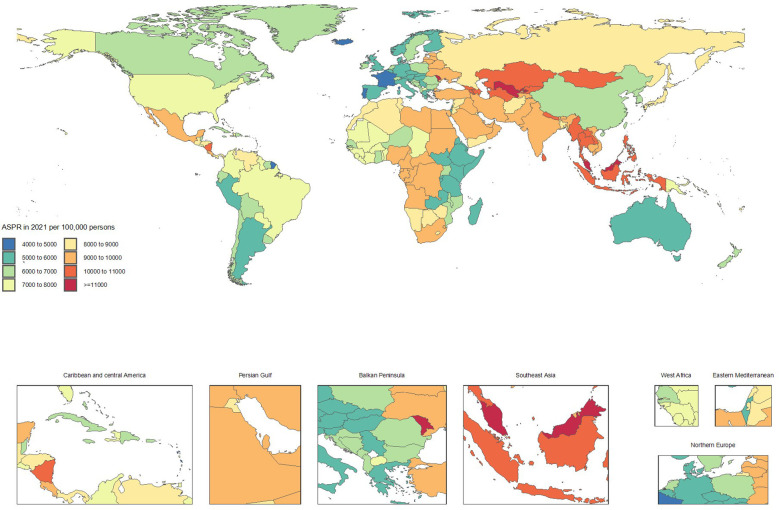
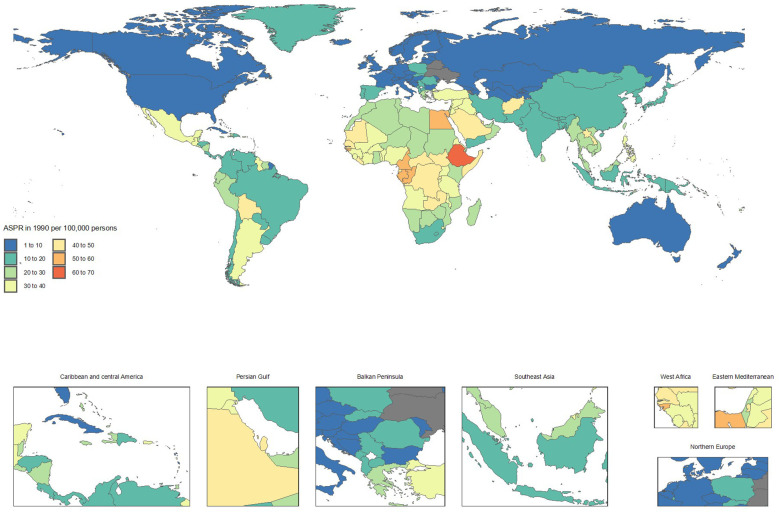
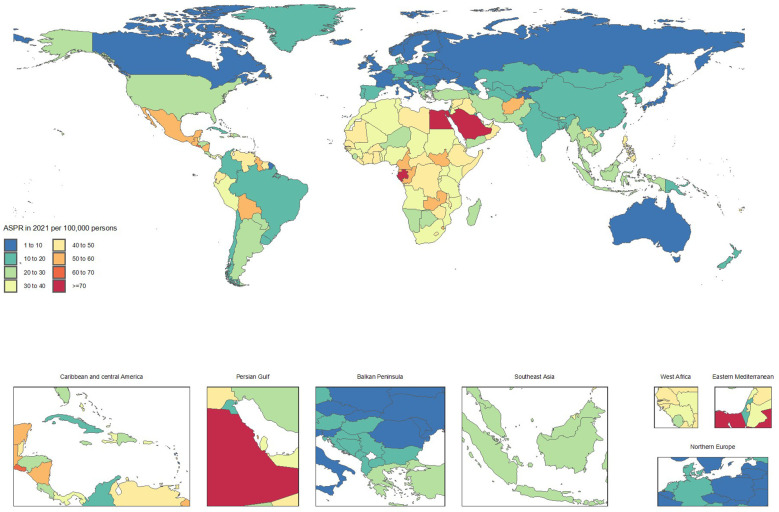
Methods: Data from the Global Burden of Disease Study (1990-2021) covering 204 countries were analyzed to assess trends in prevalence, mortality, and disability-adjusted life years for chronic kidney disease, alongside geographic, age, sex, and risk factor patterns.
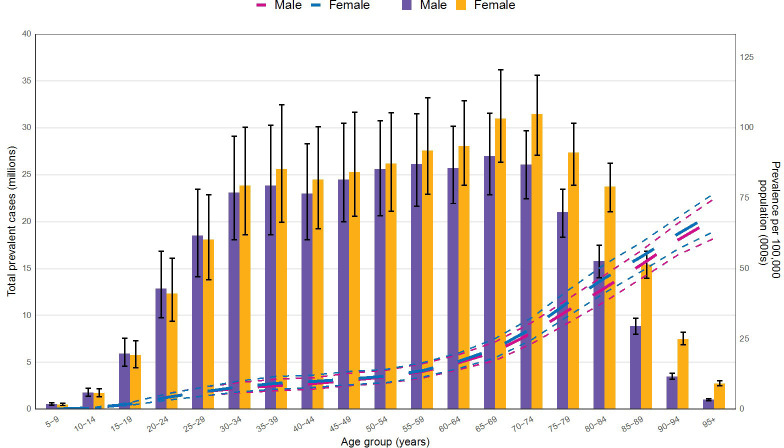
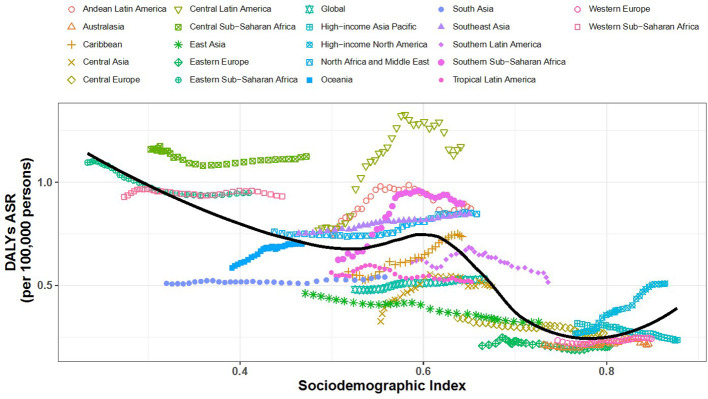
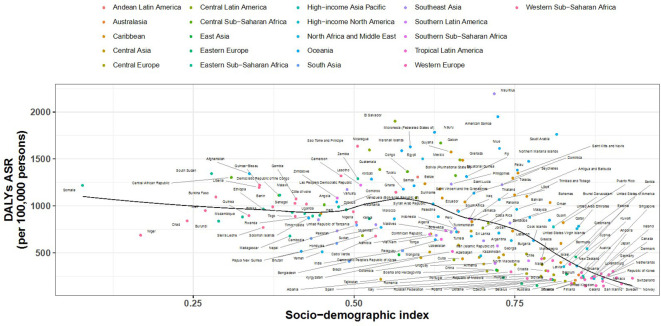
Findings: In 2021, an estimated 674 million individuals were affected globally. Although the global age-standardized prevalence rate declined slightly by 0.8% since 1990, substantial disparities persisted. High-income North America's prevalence remained stable yet showed high mortality (20.6 per 100,000) and increased DALYs (508.8 per 100,000). In contrast, East Asia's prevalence fell by 11.7%, accompanied by notable reductions in mortality (11.1 per 100,000) and DALYs (322.4 per 100,000). Regions with low socio-demographic indices, including parts of sub-Saharan Africa and South Asia, bore the greatest burdens, with persistently high prevalence (exceeding 9000 per 100,000) and rising DALYs. Some countries, such as Guatemala, experienced rapid prevalence increases, while others, like Italy, achieved substantial reductions. Similarly, mortality trends varied: Ukraine saw steep increases, while Poland showed marked improvements. DALY burdens also diverged, with El Salvador experiencing large increases, and Kuwait recording significant declines. Prevalence peaked at ages 65-69 in males and 70-74 in females, with female rates surpassing male rates from the early thirties onward. High fasting plasma glucose contributed 36% of DALYs globally, heavily affecting the Caribbean and high-income North America. High systolic blood pressure and high body mass index were particularly influential in Central Europe and high-income North America, respectively. Low fruit intake strongly affected the Middle East and East Asia.
Interpretation: These findings underscore persistent global inequalities in CKD outcomes, necessitating region-specific strategies and strengthened healthcare capacity to mitigate the burden.
Keywords: chronic kidney disease; disability-adjusted life years; global burden of disease; mortality; prevalence; risk factors.
Copyright © 2025 Li, Liu, Zhang, Li, Zhang and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Anand S, Zheng Y, Montez-Rath ME, Wei WJ, Perico N, Carminati S, et al. Do attributes of persons with chronic kidney disease differ in low-income and middle-income countries compared with high-income countries? Evidence from population-based data in six countries. BMJ Global Health. (2017) 2:e000453. doi: 10.1136/bmjgh-2017-000453 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical