

Safety and Tolerability of Brexpiprazole in Participants with Agitation Associated with Dementia due to Alzheimer's Disease: Pooled Analysis of Three Randomized Trials and an Extension Trial
- PMID: 40681915
- PMCID: PMC12423206
- DOI: 10.1007/s40263-025-01200-9
Safety and Tolerability of Brexpiprazole in Participants with Agitation Associated with Dementia due to Alzheimer's Disease: Pooled Analysis of Three Randomized Trials and an Extension Trial
Abstract
Background and objective: Older adults with dementia are particularly vulnerable to antipsychotic side effects. Brexpiprazole, an atypical antipsychotic, is approved in a number of countries for the treatment of agitation associated with dementia due to Alzheimer's disease. This pooled analysis aimed to evaluate the safety and tolerability of brexpiprazole in this patient population.
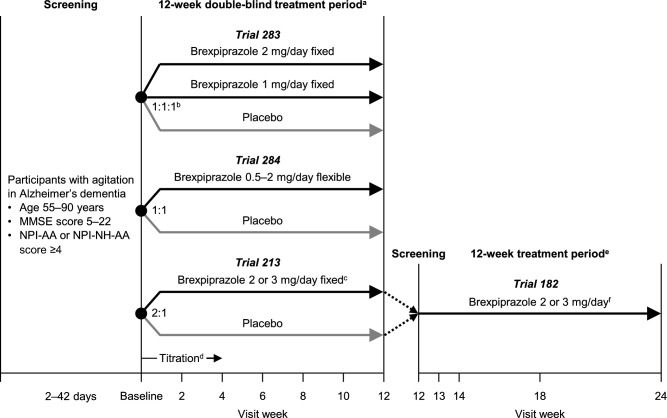
Methods: Data were included from three Phase 3, 12-week, randomized, double-blind, placebo-controlled trials and a Phase 3, 12-week, active-treatment extension trial in participants with agitation associated with dementia due to Alzheimer's disease. Safety outcomes included treatment-emergent adverse events (TEAEs), weight change, suicidality, extrapyramidal symptoms, and cognitive dysfunction. Two datasets were considered: a 12-week dataset that pooled data from the three randomized trials for brexpiprazole 0.5-3 mg/day and placebo, and a 24-week dataset that combined data from the parent randomized trial and the extension trial for brexpiprazole 2-3 mg/day.
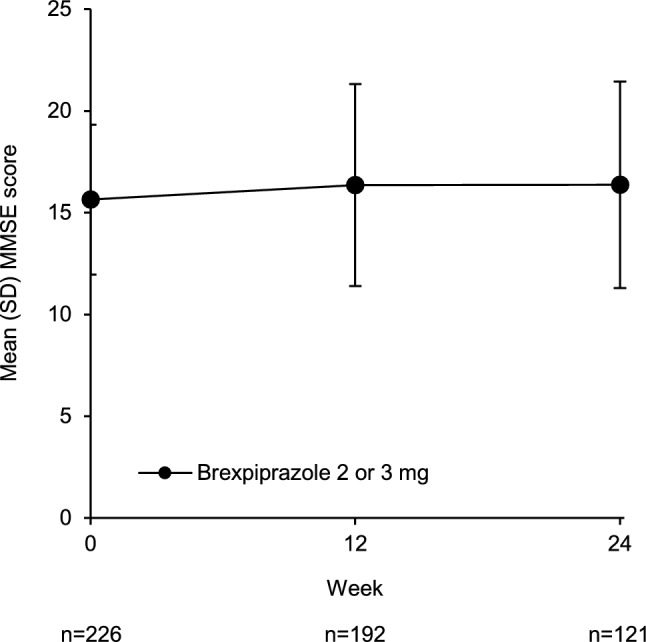
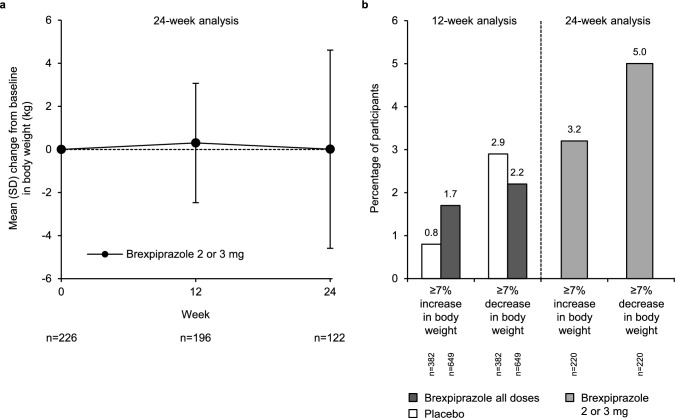
Results: Over 12 weeks, 335/655 (51.1%) participants on brexpiprazole and 178/388 (45.9%) participants on placebo reported ≥ 1 TEAE, which led to discontinuation in 41 (6.3%) and 13 (3.4%) participants, respectively. Headache was the only TEAE with incidence ≥ 5% (brexpiprazole, 50 [7.6%] participants; placebo, 36 [9.3%] participants). The incidences of cerebrovascular TEAEs (brexpiprazole, 0.5%; placebo, 0.3%), cardiovascular TEAEs (3.7%; 2.3%), extrapyramidal symptom-related TEAEs (5.3%; 3.1%), and somnolence/sedation TEAEs (3.7%; 1.8%) were generally similar between treatment groups. Six (0.9%) participants on brexpiprazole and 1 (0.3%) participant on placebo died; causes of death were not considered related to brexpiprazole and were generally in line with those expected in Alzheimer's disease. Over 24 weeks, 110/226 (48.7%) participants on brexpiprazole reported ≥ 1 TEAE, which led to discontinuation in 19 (8.4%) participants. Headache was the only TEAE with incidence ≥ 5% (18 [8.0%] participants). No participants died during the extension trial. Over 12 and 24 weeks, mean changes in weight, suicidality, and extrapyramidal symptoms were minimal, with no worsening of cognition.
Conclusions: Considering pooled data from > 1000 participants on brexpiprazole or placebo, brexpiprazole appears to be generally well tolerated for up to 24 weeks in participants with agitation associated with dementia due to Alzheimer's disease.
Study registration: ClinicalTrials.gov identifiers: NCT01862640, NCT01922258, NCT03548584, NCT03594123.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Funding: This work was supported by Otsuka Pharmaceutical Development & Commercialization Inc. (Princeton, NJ, USA) and H. Lundbeck A/S (Valby, Denmark). The sponsors were involved in the design of the research, the analysis and interpretation of data, and the writing and reviewing of this article. The sponsors paid the open access fee. Conflicts of interest: Alpesh Shah, Dalei Chen, Denise Chang, Mary Slomkowski, Mary Hobart, and Malaak Brubaker are full-time employees of Otsuka Pharmaceutical Development & Commercialization Inc. Alvin Estilo, Daniel Lee, and Saloni Behl were full-time employees of Otsuka Pharmaceutical Development & Commercialization Inc. at the time of this work. Pamela L. Sheridan was a full-time employee of Lundbeck LLC at the time of this work. Uwa Kalu is a full-time employee of Lundbeck LLC. Nanco Hefting and Pedro Such are full-time employees of H. Lundbeck A/S. George T Grossberg has received consulting fees from Acadia, Abbott, Axsome, Biogen, BMS, BioXcel, Eisai, Karuna, Lundbeck, MapLight Therapeutics, Otsuka, and Takeda. George T. Grossberg is on the Editorial Board for CNS Drugs, Journal of the American Medical Directors Association, and International Journal of Alzheimer’s Disease; he was not involved in the selection of peer reviewers for this manuscript nor any of the subsequent editorial decisions. He is on Safety Monitoring Committees for Anavex, Quince, Merck, Newron, and Oligomerix. Availability of data and material: To submit inquiries related to Otsuka clinical research, or to request access to individual participant data (IPD) associated with any Otsuka clinical trial, please visit https://clinical-trials.otsuka.com/ . For all approved IPD access requests, Otsuka will share anonymized IPD on a remotely accessible data sharing platform. Ethics approval: This analysis used pooled data from published clinical trials. The trials were approved by relevant institutional review boards and independent ethics committees and were performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments. Code availability: Not applicable. Consent to publish: Not applicable. Consent to participate: This analysis used pooled data from published clinical trials. All participants and/or their legal representatives provided written or electronic informed consent prior to the start of the trials. Author contributions: All authors contributed to the study conception and design. Data analysis was performed by Dalei Chen and Denise Chang. All authors critically reviewed the manuscript for intellectual content. All authors read and approved the final manuscript.
Figures
References
-
- Antonsdottir IM, Smith J, Keltz M, Porsteinsson AP. Advancements in the treatment of agitation in Alzheimer’s disease. Expert Opin Pharmacother. 2015;16(11):1649–56. 10.1517/14656566.2015.1059422. - PubMed
-
- Cloak N, Schoo C, Al Khalili Y. Behavioral and psychological symptoms in dementia. 2024 [cited 2024 July 30]; Available from: https://www.ncbi.nlm.nih.gov/books/NBK551552/ - PubMed
-
- Brodaty H, Arasaratnam C. Meta-analysis of nonpharmacological interventions for neuropsychiatric symptoms of dementia. Am J Psychiatry. 2012;169(9):946–53. 10.1176/appi.ajp.2012.11101529. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
