

Risk factors for different cement distribution indexes for refracture of operated vertebrae and adjacent vertebrae after percutaneous vertebroplasty in patients with thoracolumbar compression fracture
- PMID: 40682022
- PMCID: PMC12275346
- DOI: 10.1186/s12893-025-03033-1
Risk factors for different cement distribution indexes for refracture of operated vertebrae and adjacent vertebrae after percutaneous vertebroplasty in patients with thoracolumbar compression fracture
Abstract
Background: Although most studies suggest that unilateral percutaneous vertebroplasty (PVP) increases the probability of secondary adjacent vertebral compression fractures, controversy remains the associated risk factors.
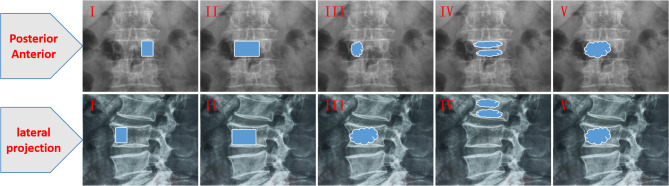
Objective: To explore the risk factors of bone cement distribution index (DI) for surgical and adjacent vertebrae after PVP.
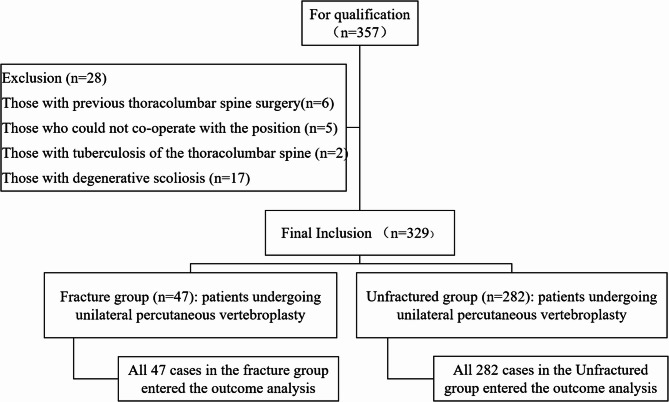
Methods: According to the inclusion criteria, 329 patients who underwent PVP in the Spinal Surgery Department of the Sixth Affiliated Hospital of Xinjiang Medical University between January 2018 and May 2024 were then retrospectively screened, and the patients were divided into two groups based on whether refracture occurred during the follow-up period. The two groups were (1) fracture group (n = 47) and (2) no fracture group (n = 282). The following variables were reviewed in both groups: age, gender, body mass index (BMI), PVP segment, cement leakage, bone density, T, cement dose, smoking, drinking, hypertension, type 2 diabetes mellitus, COPD, cerebral hemorrhage, coronary heart disease, cement DI type, chronic kidney history and previous fracture (caused by osteoporosis). These factors were univariate analyzed and replaced P < 0.05 with binary Logistic analysis to explore the factors associated with postoperative vertebral recompression fracture.
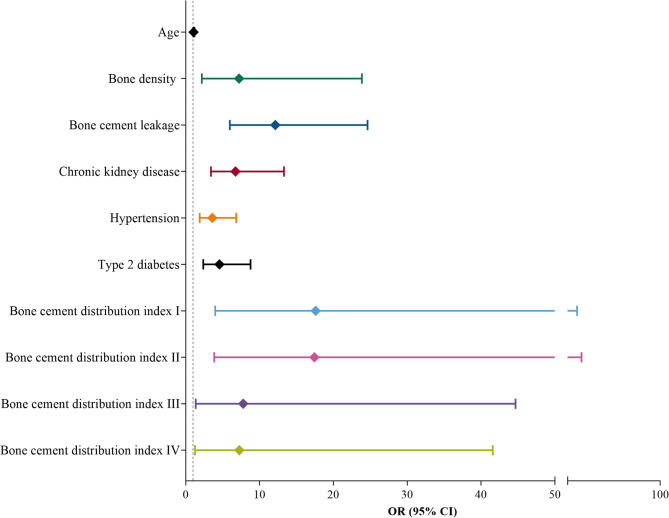
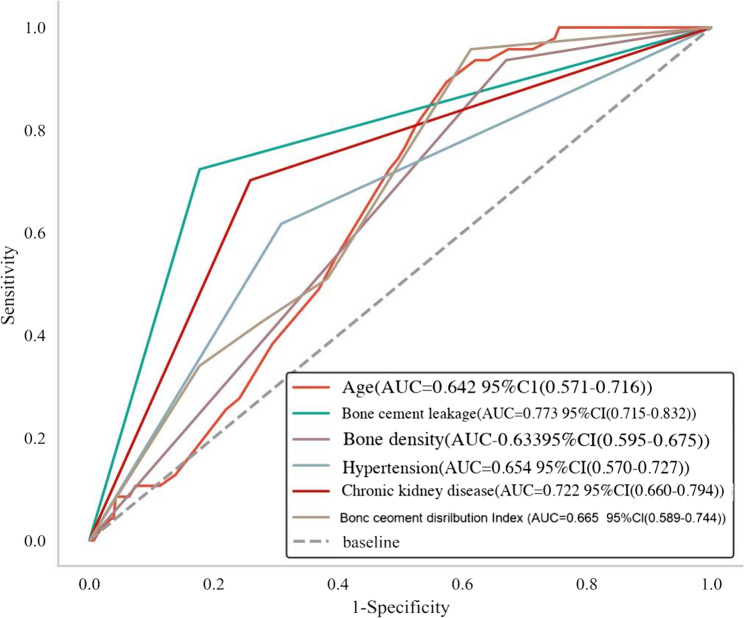
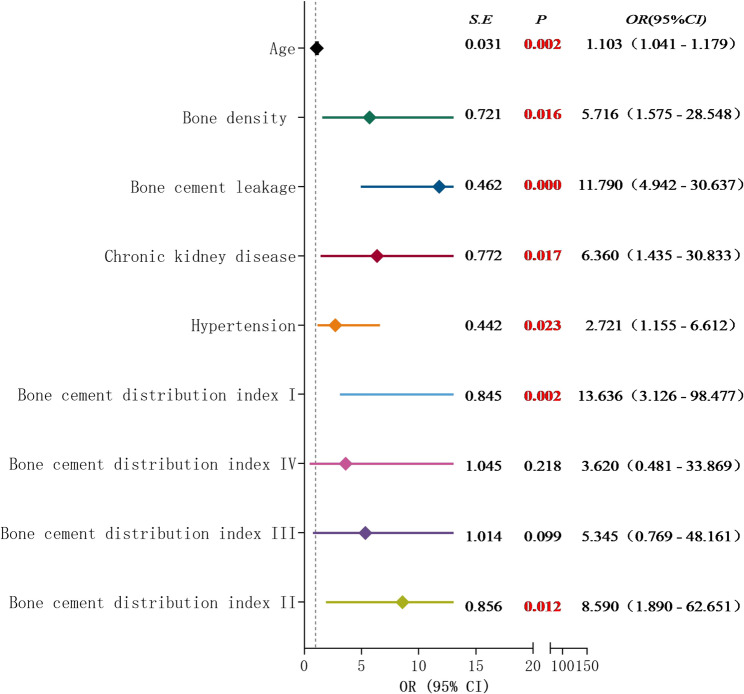
Results: A total of 329 patients were included in this study to compare the parameters between the fracture and nonfracture groups. The results of univariate analysis showed that postoperative vertebral refracture was related to age, cement leakage, bone mineral density T value, history of hypertension, history of type 2 diabetes mellitus, the index type of bone cement distribution, and chronic kidney disease, and the difference was statistically significant (P < 0.05). By binary Logistic regression, Age (OR = 1.103, 95%CI:1.041-1.179, P = 0.002), leakage of bone cement (OR = 11.790,95%CI:4.942-30.637,P < 0.001) MD T value (OR = 5.716, 95%CI: 1.575-28.548, P = 0.016), history of hypertension (OR = 2.721, 95%CI:1.155-6.612, P = 0.023), history of chronic kidney disease (OR = 6.360, 95%CI:1.435-30.833, P = 0.017), type I bone cement DI [OR = 13.636, 95%CI: 3.126-98.477, P = 0.002] and type II cement DI [OR = 8.590, 95%CI:1.890-62.651, P = 0.012] was a risk factor for refracture of the operated and adjacent vertebrae.
Conclusion: The results showed that age, cement leakage, bone mineral density T value, history of hypertension, and cement DI type were risk factors for refracture of the operated vertebrae and adjacent vertebrae. The surgeon conducts a comprehensive evaluation of patients before surgery, which can more accurately estimate the probability of fracture again, and then provide a reference for the formulation of personalized treatment plan, so as to reduce the risk of fracture again in the future.
Keywords: Distribution index; Osteoporotic vertebral compression fracture; Percutaneous vertebroplasty; Risk factors; The adjacent vertebral body fracture; Vertebral body recompression.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: We confrm that all experiments were performed in accordance with the Declaration of Helsinki. The study was approved by the Ethical Committee of the Sixth Afliated Hospital of Xinjiang Medical University, NO. LFYLLSC20230510-01. Each patient provided written informed consent before participating in the study. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Xu J, Zhai T. Coffee Drinking and the Odds of Osteopenia and Osteoporosis in Middle-Aged and Older Americans: A Cross-Sectional Study in NHANES 2005–2014. Calcif Tissue Int. 2024;114(4):348–59. - PubMed
-
- Felsenberg D, Silman AJ, Lunt M, et al. Incidence of vertebral fracture in europe: results from the European Prospective Osteoporosis Study (EPOS). J Bone Miner Res. 2002;17(4):716–24. - PubMed
-
- Pongchaiyakul C, Charoensri S, Leerapun T, et al. Prevalence of asymptomatic radiographic vertebral fracture in postmenopausal Thai women. Arch Osteoporos. 2020;15(1):78. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
