

Hypnosis for unplanned procedural pain in the intensive care unit: the HYPIC randomized clinical trial
- PMID: 40682163
- PMCID: PMC12275327
- DOI: 10.1186/s13054-025-05563-9
Hypnosis for unplanned procedural pain in the intensive care unit: the HYPIC randomized clinical trial
Abstract
Background: Pain and anxiety are frequent among critically ill patients undergoing unplanned invasive procedures, and pharmacological pain relief is not always possible. Although hypnosis is widely used in planned painful procedures, studies are lacking in this specific setting. Thus, we aimed to assess whether hypnosis plus standard care reduced pain and anxiety in critically ill patients undergoing an unplanned invasive procedure in comparison to standard care.
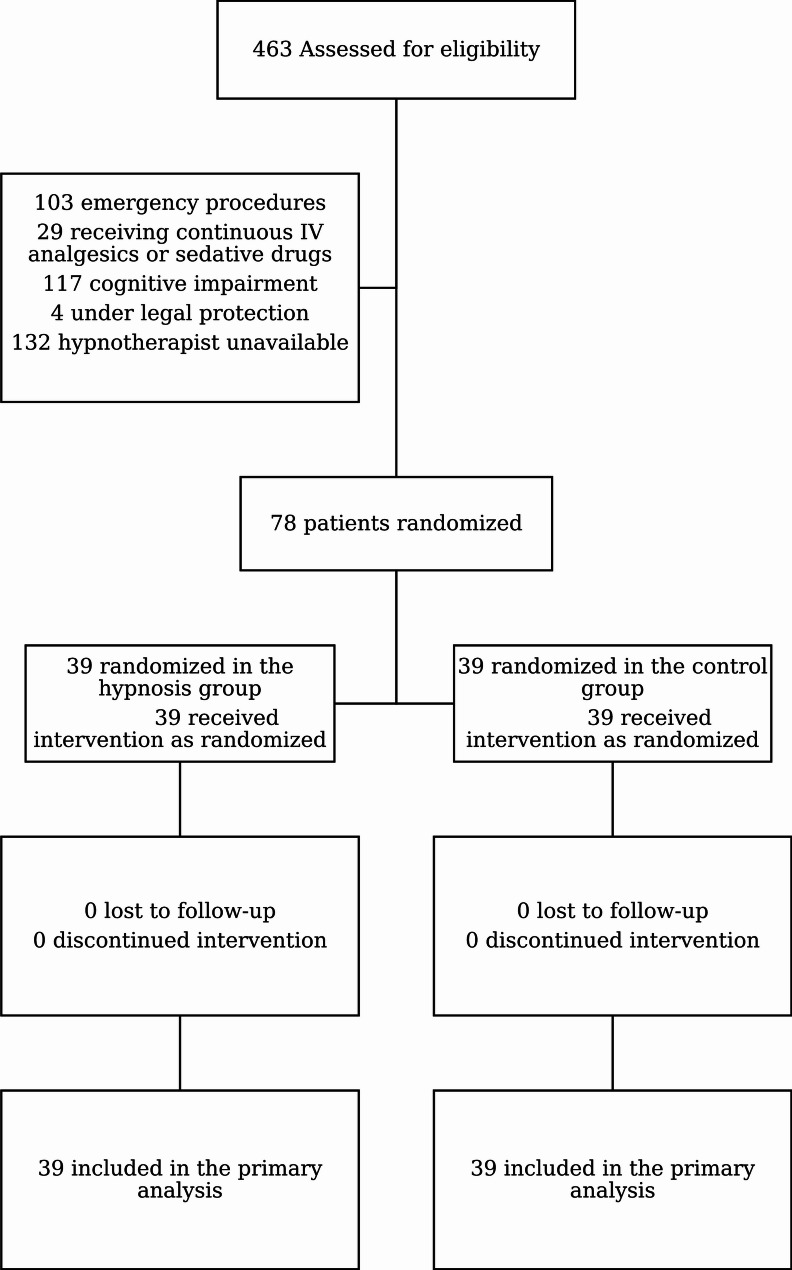
Methods: The HYPIC trial was a randomized, single-blind, multicenter clinical trial of hypnosis during unplanned invasive procedures versus standard care for critically ill patients conducted in two French intensive care units (ICUs) from December 27, 2019, to January 25, 2022. Patients were randomly assigned to receive hypnosis plus standard care by trained healthcare providers or standard care. The hypnotherapists were in the room for both arms to maintain blindness. The primary endpoint was the difference in pain level experienced during the invasive procedure assessed immediately after the end of the procedure between the two groups. The secondary outcomes were anxiety level, lidocaine consumption and stress experienced by the ICU nurses in charge of the patients.
Results: We included 78 patients. The pain level, assessed with a numeric pain scale (range, 0-10), was not significantly different between the two groups (2.2 ± 2.9 vs. 2.2 ± 3, difference 0 pts [95% CI -1.3; 1.3], p = 0.89). The level of anxiety was significantly lower in the hypnosis group (2.4 ± 2.8 vs. 4.1 ± 3, difference - 1.7 [-3; -0.4], p = 0.01), as was the level of stress experienced by the ICU nurses (0.1 ± 0.4 vs. 0.9 ± 1.5, difference - 0.8 [-1.3;-0.3], p = 0.003), and the patients were three times less likely to require increased lidocaine consumption (odds ratio: 0.3 [0.13-0.84], p = 0.02) in the hypnosis group.
Conclusion: While hypnosis did not result in a statistically significant reduction in unplanned procedural pain, it seems to reduce anxiety, increase comfort, and reduce the stress level of healthcare providers.
Trial registration: The study was registered on ClinicalTrials.gov (NCT04129333) on 14 October 2019, before the first patient was enrolled.
Keywords: Catheter placement; Chest tube; Critical illness; Hypnosis; Intensive care unit; Randomized controlled trial.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The trial was approved for all centers by a central Ethics Committee (IDCRB 2019-A01775-52, Comité de Protection des Personnes Bron —Région SUD-EST II, France) according to French law on October 9, 2019. This study was conducted in accordance with the ethical standards of the Declaration of Helsinki and the Good Clinical Practice requirements. Written informed consent was required for all patients prior to enrollment and randomization. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


References
-
- Pottier V, Daubin C, Lerolle N, Gaillard C, Viquesnel G, Plaud B, et al. Overview of adverse events related to invasive procedures in the intensive care unit. Am J Infect Control. 2012;40:241–6. - PubMed
-
- Devlin JW, Skrobik Y, Gélinas C, Needham DM, Slooter AJC, Pandharipande PP, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46:e825–73. - PubMed
-
- Puntillo KA, Max A, Timsit J-F, Vignoud L, Chanques G, Robleda G, et al. Determinants of procedural pain intensity in the intensive care unit. The Europain® study. Am J Respir Crit Care Med. 2014;189:39–47. - PubMed
-
- Amraoui J, Pouliquen C, Fraisse J, Dubourdieu J, Rey Dit Guzer S, Leclerc G, et al. Effects of a hypnosis session before general anesthesia on postoperative outcomes in patients who underwent minor breast Cancer surgery: the HYPNOSEIN randomized clinical trial. JAMA Netw Open. 2018;1:e181164. - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- PHRIP-18-0299/Ministère des Affaires Sociales et de la Santé
- PHRIP-18-0299/Ministère des Affaires Sociales et de la Santé
- PHRIP-18-0299/Ministère des Affaires Sociales et de la Santé
- PHRIP-18-0299/Ministère des Affaires Sociales et de la Santé
- PHRIP-18-0299/Ministère des Affaires Sociales et de la Santé
- PHRIP-18-0299/Ministère des Affaires Sociales et de la Santé
- PHRIP-18-0299/Ministère des Affaires Sociales et de la Santé
- PHRIP-18-0299/Ministère des Affaires Sociales et de la Santé
- PHRIP-18-0299/Ministère des Affaires Sociales et de la Santé
- PHRIP-18-0299/Ministère des Affaires Sociales et de la Santé
- PHRIP-18-0299/Ministère des Affaires Sociales et de la Santé
- PHRIP-18-0299/Ministère des Affaires Sociales et de la Santé
- PHRIP-18-0299/Ministère des Affaires Sociales et de la Santé
- PHRIP-18-0299/Ministère des Affaires Sociales et de la Santé
- PHRIP-18-0299/Ministère des Affaires Sociales et de la Santé
- PHRIP-18-0299/Ministère des Affaires Sociales et de la Santé
LinkOut - more resources
Full Text Sources
Medical
