

Could Low-Value Diagnostic Tests be Compounding Access Block? A Single-Site, Cross-Sectional Study
- PMID: 40686189
- PMCID: PMC12278031
- DOI: 10.1111/1742-6723.70100
Could Low-Value Diagnostic Tests be Compounding Access Block? A Single-Site, Cross-Sectional Study
Abstract
Objective: The study aimed to evaluate the prevalence and impact of low-value diagnostic tests at a regional, major-referral, mixed Emergency Department (ED).
Methods: A single-site, cross-sectional study was conducted at Townsville University Hospital in April 2022. Adult patients (aged 18 years and above) who underwent one of 10 specified diagnostic tests were included. The tests encompassed coagulation studies, urine cultures, blood cultures, cranial computed tomography (CT) in syncope, cranial CT in minor head injury, cervical spine CT in neck trauma, ankle X-ray in acute ankle trauma, duplex lower extremity ultrasound in suspected deep vein thrombosis, CT pulmonary angiography in suspected pulmonary embolism, and CT kidney ureter bladder in renal colic. Tests were classified as low-value based on Choosing Wisely recommendations, with their value determined by a research assistant using clinical documentation, prior to the availability of test results. Emergency clinicians were blinded to the study conduct.
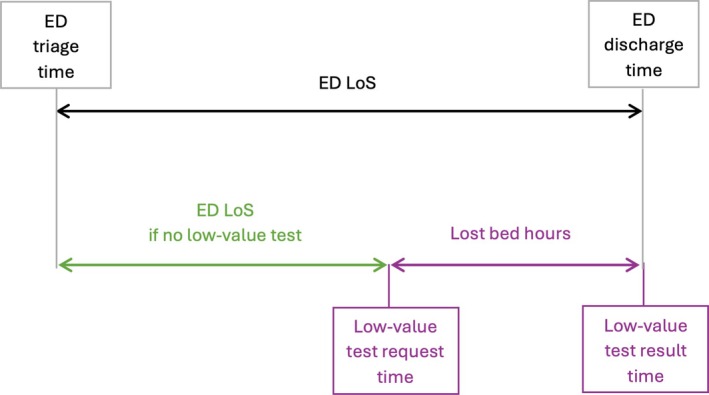
Results: Of all diagnostic tests performed, 48.2% (276/572) were deemed low-value, including 50.6% of laboratory tests (246/486) and 24.4% of imaging tests (21/86). The median ED length of stay was 6.1 h (IQR 3.9-8.5). Low-value imaging tests contributed to 152 lost bed-hours per 100 tests.
Conclusion: A substantial proportion of diagnostic tests were low-value, exacerbating access block and reducing the availability of ED beds, thereby delaying timely emergency care. The implementation of evidence-based, effective strategies is imperative to mitigate patient harm associated with low-value diagnostic tests.
Keywords: access block; diagnostic tests; emergency medicine; low‐value care.
© 2025 The Author(s). Emergency Medicine Australasia published by John Wiley & Sons Australia, Ltd on behalf of Australasian College for Emergency Medicine.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
PECARN prediction rule for cervical spine imaging of children presenting to the emergency department with blunt trauma: a multicentre prospective observational study.Lancet Child Adolesc Health. 2024 Jul;8(7):482-490. doi: 10.1016/S2352-4642(24)00104-4. Epub 2024 Jun 4. Lancet Child Adolesc Health. 2024. PMID: 38843852 Free PMC article.
-
Systematic review and validation of prediction rules for identifying children with serious infections in emergency departments and urgent-access primary care.Health Technol Assess. 2012;16(15):1-100. doi: 10.3310/hta16150. Health Technol Assess. 2012. PMID: 22452986 Free PMC article.
-
Diagnostic tests and algorithms used in the investigation of haematuria: systematic reviews and economic evaluation.Health Technol Assess. 2006 Jun;10(18):iii-iv, xi-259. doi: 10.3310/hta10180. Health Technol Assess. 2006. PMID: 16729917
-
Diagnostic Accuracy of History, Physical Examination, Laboratory Tests, and Point-of-care Ultrasound for Pediatric Acute Appendicitis in the Emergency Department: A Systematic Review and Meta-analysis.Acad Emerg Med. 2017 May;24(5):523-551. doi: 10.1111/acem.13181. Acad Emerg Med. 2017. PMID: 28214369
-
Diagnostic management strategies for adults and children with minor head injury: a systematic review and an economic evaluation.Health Technol Assess. 2011 Aug;15(27):1-202. doi: 10.3310/hta15270. Health Technol Assess. 2011. PMID: 21806873 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
