

Semi-automated tortuosity measurements confirm generalizability of IMPERATIVE trial results to real-world patients with acute ischemic stroke undergoing thrombectomy
- PMID: 40686305
- PMCID: PMC12279764
- DOI: 10.1177/15910199251359089
Semi-automated tortuosity measurements confirm generalizability of IMPERATIVE trial results to real-world patients with acute ischemic stroke undergoing thrombectomy
Abstract
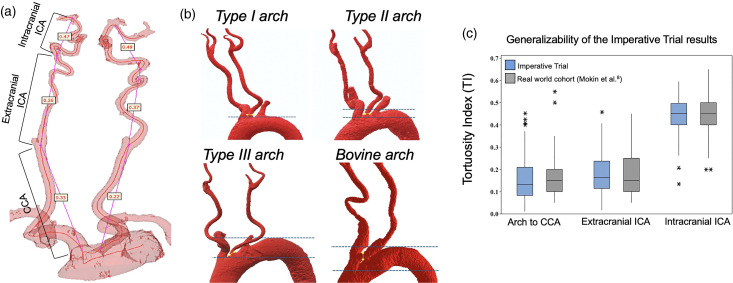
BackgroundCriticism of clinical trials of endovascular therapy of acute ischemic stroke due to large vessel occlusion includes their lack of generalizability. We aimed to evaluate the impact of vessel tortuosity on the outcomes of large-bore and super-bore aspiration catheters in the Imperative Trial and to compare trial's selection of patients to a real-world setting.MethodsUsing baseline craniocervical angiography, we performed semi-automated analysis of various tortuosity characteristics. Comparison of tortuosity characteristics was made to a previously published cohort of 100 consecutive patients treated with thrombectomy (real-world cohort).ResultsOf the 249 Imperative Trial patients with anterior circulation strokes, 187 (89%) had complete tortuosity assessments from the aortic arch to the occlusion site. Tortuosity indexes for the common carotid, extracranial and intracranial internal carotid artery segments were similar for both cohorts (right side 0.18 ± 0.10, 0.17 ± 0.09, 0.45 ± 0.09 vs. 0.20 ± 0.09, 0.17 ± 0.09, 0.45 ± 0.09; left side: 0.12 ± 0.08, 0.19 ± 0.09, 0.44 ± 0.07 vs. 0.15 ± 0.08, 0.18 ± 0.08, 0.47 ± 0.07 in the Imperative Trial and in the real-world cohort, respectively). The proportion of patients with type 3 aortic arches was higher in the Imperative Trial than the real-word cohort (26% vs. 15%, p = .038).ConclusionsImperative trial patients treated with aspiration thrombectomy had similar vascular tortuosity characteristics compared to patients treated with thrombectomy in a real-world clinical setting. This confirms the generalizability of Imperative Trial findings to real-world clinical practice.
Keywords: CTA; Stroke; aspiration; thrombectomy; tortuosity.
Figures

Similar articles
-
Cost-Effectiveness of Endovascular Thrombectomy in M2 Occlusion Stroke: Real-World Experience Versus Clinical Trials.J Endovasc Ther. 2025 Aug;32(4):1047-1055. doi: 10.1177/15266028231201098. Epub 2023 Oct 3. J Endovasc Ther. 2025. PMID: 37789615 Free PMC article.
-
Intravenous thrombolytic treatment and endovascular thrombectomy for ischaemic wake-up stroke.Cochrane Database Syst Rev. 2021 Dec 1;12(12):CD010995. doi: 10.1002/14651858.CD010995.pub3. Cochrane Database Syst Rev. 2021. PMID: 34850380 Free PMC article.
-
Efficacy and safety of nerinetide in acute ischaemic stroke in patients undergoing endovascular thrombectomy without previous thrombolysis (ESCAPE-NEXT): a multicentre, double-blind, randomised controlled trial.Lancet. 2025 Feb 15;405(10478):560-570. doi: 10.1016/S0140-6736(25)00194-1. Lancet. 2025. PMID: 39955119 Clinical Trial.
-
Trial of Endovascular Thrombectomy for Large Ischemic Strokes.N Engl J Med. 2023 Apr 6;388(14):1259-1271. doi: 10.1056/NEJMoa2214403. Epub 2023 Feb 10. N Engl J Med. 2023. PMID: 36762865 Clinical Trial.
-
Duplex ultrasound for diagnosing symptomatic carotid stenosis in the extracranial segments.Cochrane Database Syst Rev. 2022 Jul 11;7(7):CD013172. doi: 10.1002/14651858.CD013172.pub2. Cochrane Database Syst Rev. 2022. PMID: 35815652 Free PMC article.
References
-
- Mokin M, Ansari SA, McTaggart RA, et al. Indications for thrombectomy in acute ischemic stroke from emergent large vessel occlusion (ELVO): report of the SNIS standards and guidelines committee. J Neurointerv Surg 2019; 11: 215–220. - PubMed
-
- Turc G, Bhogal P, Fischer U, et al. European stroke organisation (ESO): European society for minimally invasive neurological therapy (ESMINT) guidelines on mechanical thrombectomy in acute ischemic stroke. J Neurointerv Surg 2023; 15: e8. - PubMed
-
- Qureshi AI, Singh B, Huang W, et al. Mechanical thrombectomy in acute ischemic stroke patients performed within and outside clinical trials in the United States. Neurosurgery 2020; 86: E2–E8. - PubMed
LinkOut - more resources
Full Text Sources
