

The optimal montage to mark interictal epileptiform discharges and high-frequency oscillations in intraoperative electrocorticography
- PMID: 40687074
- PMCID: PMC12272942
- DOI: 10.1016/j.cnp.2025.06.007
The optimal montage to mark interictal epileptiform discharges and high-frequency oscillations in intraoperative electrocorticography
Abstract
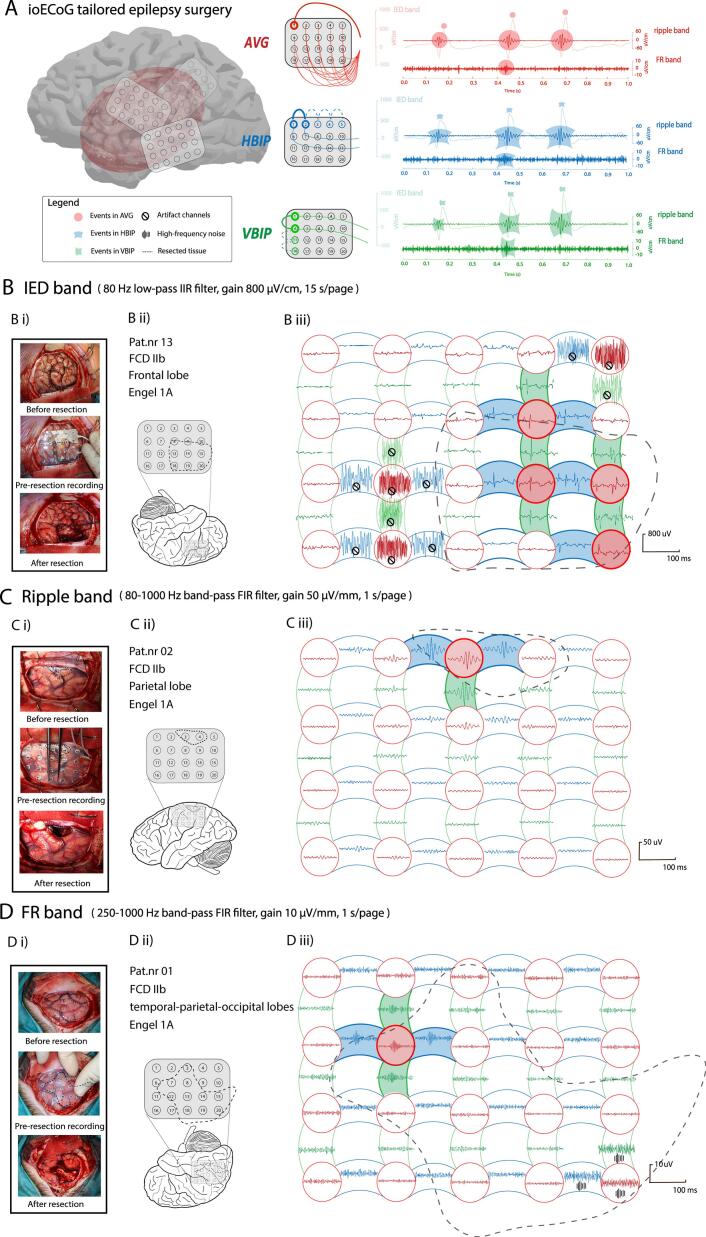
Objective: In intraoperative electrocorticography (ioECoG), interictal epileptiform discharges (IEDs) and high-frequency oscillations (HFOs; ripples 80-250 Hz, fast ripples (FRs) 250-500 Hz) can be identified in average or bipolar montage. We studied how montage choice affects event identification.
Methods: Two reviewers independently marked IEDs and HFOs across three montages (average, horizontal- and vertical-bipolar) from 13 patients who were seizure-free after ioECoG-guided surgery. We analyzed the number of channels-with-events, total events count, events morphology (maximum-amplitude, duration, frequency), number of instances with overlapping events across multiple channels (event_instance), concordance of event_instances over montages, and percentage of channels-with-events in the resected-area.
Results: Bipolar montages yielded more channels-with-events, higher counts, and greater maximum-amplitude of IEDs and ripples compared to average montages. Average and horizontal-bipolar montages yielded more IED_instances than vertical-bipolar montages. Average montages detected the highest percentage of event_instances occurring only in this montage. Event duration, frequency, and percentage of channels-with-events in the resected-area did not differ across montages.
Conclusions: All three ioECoG montages are clinically useful to find epileptic events. The bipolar montage detects more events with greater amplitude, while the average montage uncovers a wider variety of unique events. Combining montages provides complementary information.
Significance: This study quantitatively revealed how different montages capture epileptiform events.
Keywords: Electrode grid; Epilepsy surgery; High-frequency oscillations; Intraoperative electrocorticography; Montage.
© 2025 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

References
-
- Acharya J.N., Acharya V.J. Overview of EEG montages and principles of localization. J. Clin. Neurophysiol. 2019;36(5):325–329. - PubMed
-
- Acharya J.N., Hani A.J., Thirumala P.D., Tsuchida T.N. American clinical neurophysiology society guideline 3: a Proposal for standard montages to be used in clinical EEG. J. Clin. Neurophysiol. 2016;33(4):312–316. - PubMed
-
- Alarcon G., Garcia Seoane J.J., Binnie C.D., Martin Miguel M.C., Juler J., Polkey C.E., et al. Origin and propagation of interictal discharges in the acute electrocorticogram. Implications for pathophysiology and surgical treatment of temporal lobe epilepsy. Brain. 1997;120(Pt 12):2259–2282. - PubMed
-
- Boran E., Ramantani G., Krayenbühl N., Schreiber M., König K., Fedele T., Sarnthein J. High-density ECoG improves the detection of high frequency oscillations that predict seizure outcome. Clin. Neurophysiol. 2019;130(10):1882–1888. - PubMed
LinkOut - more resources
Full Text Sources
