

Knee Pain Expansion in Early Osteoarthritis: Findings from Iwaki Cohort Study
- PMID: 40687334
- PMCID: PMC12276747
- DOI: 10.2147/JPR.S526036
Knee Pain Expansion in Early Osteoarthritis: Findings from Iwaki Cohort Study
Abstract
Purpose: In advanced knee osteoarthritis (KOA), chronic pain contributes to central sensitization, amplifying pain perception. Few studies have evaluated pain expansion in early-phase KOA. Here, we investigated how the pain area expands with KOA severity and its association with other knee symptoms.
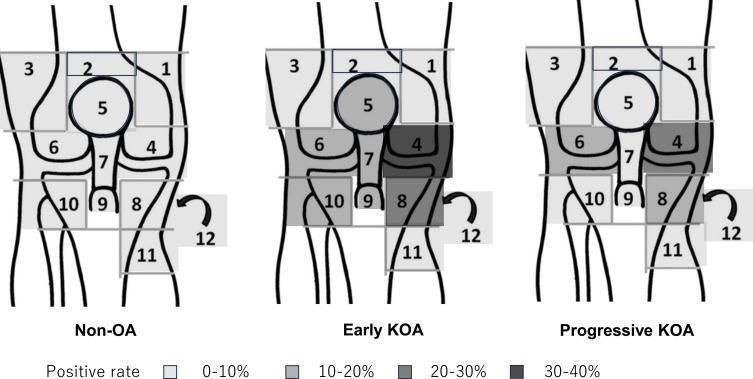
Patients and methods: Among 737 community-dwelling volunteers, 658 were enrolled. Early KOA was defined according to Luyten's classification, and progressive KOA was defined as Kellgren-Lawrence ≥grade 2. A knee diagram, divided into 12 sections corresponding to the knee anatomy, was marked by patients to indicate areas of pain. The number of sections with reported pain was scored for analysis. Knee symptoms were evaluated using the Knee injury and Osteoarthritis Outcome Scales (KOOS), and their relationship with the number of pain-positive sections was analyzed.
Results: Of 658 subjects, 38 had early KOA and 233 had progressive KOA. The mean number of pain-positive sections was significantly higher in early KOA and progressive KOA groups than in normal knee (1.5, 1.0, and 0.3, respectively; p< 0.001). The anterior medial section (medial joint line and medial collateral ligament) was most frequently affected, followed by the pes anserinus and anterolateral region (lateral joint line and lateral collateral ligament) in overall participants. The number of indicated pain-positive sections correlated negatively with the KOOS scores. ROC analysis to estimate the KOOS total score cutoff for detecting the presence of two or more positive sections revealed a cutoff of 475 points for pain expansion, with a sensitivity of 0.310, a specificity of 0.846, and an [OR] of 12.21. (p ≤ 0.001, AUC: 0.828).
Conclusion: Individuals with early KOA perceived more expansive pain areas than those with normal knees or progressive KOA. Expansion of the pain area was associated with knee symptom. Investigating the expansion of the pain sections may be useful in diagnosis for early KOA.
Keywords: early knee osteoarthritis; knee osteoarthritis; pain drawing.
© 2025 Tomita et al.
Conflict of interest statement
The authors declare that they have no competing interests in this work.
Figures




References
LinkOut - more resources
Full Text Sources
