

Primary aldosteronism patients with bilateral adrenal vein sampling success achieve better outcomes through unilateral adrenalectomy
- PMID: 40687666
- PMCID: PMC12271940
- DOI: 10.21037/tau-2025-89
Primary aldosteronism patients with bilateral adrenal vein sampling success achieve better outcomes through unilateral adrenalectomy
Abstract
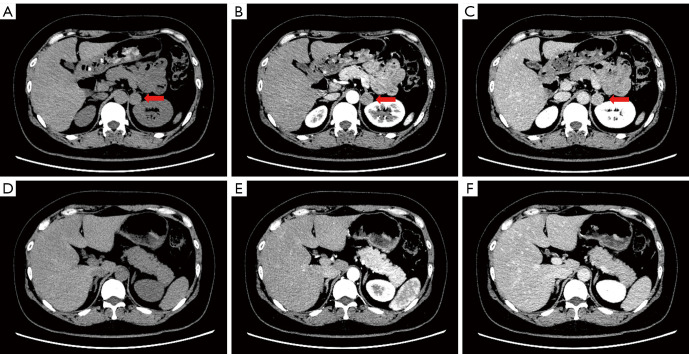
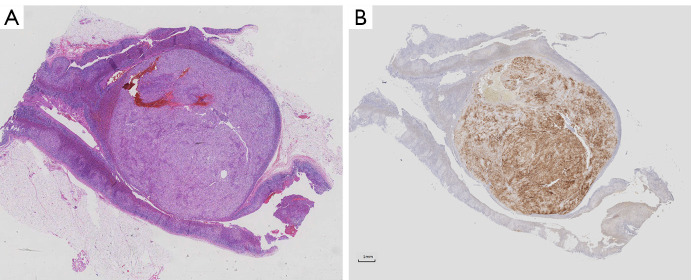
Background: Adrenal vein sampling (AVS) is the gold standard for diagnosing the dominant side in patients with primary aldosteronism (PA). CYP11B2 encodes aldosterone synthase. The aim of this study was to investigate the prognosis of dominant-side adrenalectomy in patients with PA identified by AVS in the context of aldosterone synthase expression in the postoperative pathology of those patients.
Methods: This retrospective study included 73 PA patients who underwent AVS followed by unilateral adrenalectomy. Patients were categorized into AVS bilateral success group, AVS unilateral success group, and AVS bilateral failure group based on their AVS status. Immunohistochemistry (IHC) for CYP11B2 was combined with postoperative pathology in these patients, and the clinical and biochemical prognosis of these patients was assessed 6 months after adrenalectomy.
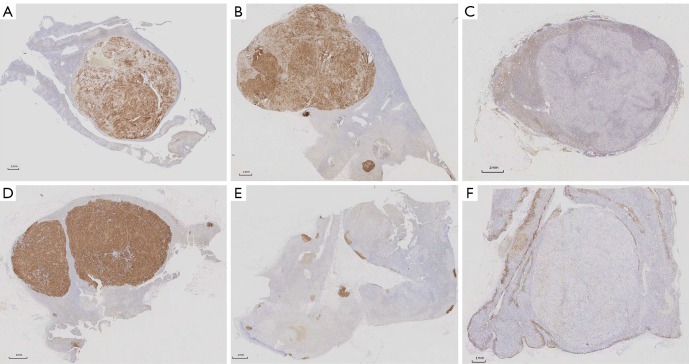
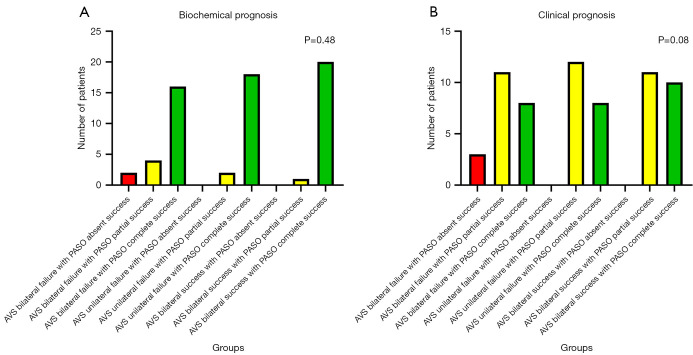
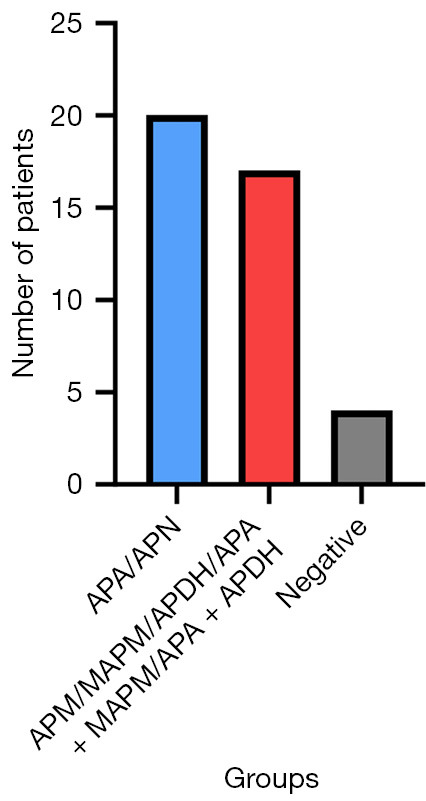
Results: Between September 2023 and September 2024, 73 patients underwent unilateral adrenalectomy guided by AVS at our institution, with CYP11B2 IHC successfully performed in 63 cases. Among these, 21 patients (33.33%) achieved bilateral AVS success, 20 (31.75%) demonstrated unilateral AVS success, and 22 (34.92%) exhibited bilateral AVS failure. Pathological analysis of the bilateral AVS success group revealed aldosterone-producing adenoma (APA) in 12 cases, aldosterone-producing micronodule (APM) in 1, multiple-aldosterone-producing micronodules/nodules (MAPM/MAPN) in 2, aldosterone-producing diffuse hyperplasia (APDH) in 1, APA with MAPM in 3, and APA with APDH in 2. In this group, complete and partial clinical success rates were 47.62% (10/21) and 52.38% (11/21), respectively, while biochemical success rates reached 95.24% (20/21) for complete and 4.76% (1/21) for partial success. The unilateral AVS success cohort included APA (n=8), aldosterone-producing nodule (APN) (n=2), MAPM/MAPN (n=3), APA with MAPM (n=4), APA with APDH (n=2), and 1 CYP11B2 IHC-negative lesion, with clinical success rates of 40.00% (8/20) complete and 60.00% (12/20) partial, alongside 90.00% (18/20) complete and 10.00% (2/20) partial biochemical success. The bilateral AVS failure group comprised APA (n=8), MAPM/MAPN (n=1), APA with MAPM (n=5), APA with APDH (n=2), and 6 CYP11B2 IHC-negative lesions, demonstrating 36.36% (8/22) complete, 50.00% (11/22) partial, and 13.64% (3/22) no clinical success, with biochemical outcomes of 72.73% (16/22) complete, 18.18% (4/22) partial, and 9.09% (2/22) no success. Notably, bilateral AVS success correlated with significantly superior biochemical outcomes compared to bilateral failure (P=0.045).
Conclusions: Adrenalectomy guided by AVS yields better outcomes in patients with PA when AVS is successful on both sides compared to those with bilateral AVS failure. The source of excess aldosterone secretion on the dominant side identified by AVS is not necessarily an APA/APN. It may also include MAPM/MAPN, diffuse adrenal cortical hyperplasia, and various complex combined conditions. In patients with bilateral AVS failure, adrenal specimens more frequently exhibit negative immunohistochemical staining for CYP11B2.
Keywords: CYP11B2; Primary aldosteronism (PA); adrenal vein sampling (AVS); dominant side; prognosis.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tau.amegroups.com/article/view/10.21037/tau-2025-89/coif). The authors have no conflicts of interest to declare.
Figures

Similar articles
-
CXCR4-directed PET with 68Ga-pentixafor versus adrenal vein sampling for the diagnosis of unilateral primary aldosteronism.Endocrine. 2025 Aug;89(2):603-613. doi: 10.1007/s12020-025-04236-5. Epub 2025 May 19. Endocrine. 2025. PMID: 40388084 Free PMC article.
-
Histopathological evaluation based on CYP11B2 staining predicts outcomes in unilateral primary aldosteronism.Eur J Endocrinol. 2025 May 30;192(6):763-775. doi: 10.1093/ejendo/lvaf118. Eur J Endocrinol. 2025. PMID: 40539251
-
Total or partial adrenalectomy for aldosterone-producing adenoma: can 68Ga-Pentixafor PET/CT predict surgical outcomes?Eur J Nucl Med Mol Imaging. 2025 Aug;52(10):3632-3642. doi: 10.1007/s00259-025-07244-9. Epub 2025 Apr 4. Eur J Nucl Med Mol Imaging. 2025. PMID: 40183955 Clinical Trial.
-
Systematic review: diagnostic procedures to differentiate unilateral from bilateral adrenal abnormality in primary aldosteronism.Ann Intern Med. 2009 Sep 1;151(5):329-37. doi: 10.7326/0003-4819-151-5-200909010-00007. Ann Intern Med. 2009. PMID: 19721021
-
Subtyping of Primary Aldosteronism by Adrenal Venous Sampling.Endocr Rev. 2025 Jul 15;46(4):501-517. doi: 10.1210/endrev/bnaf007. Endocr Rev. 2025. PMID: 39965116 Free PMC article. Review.
References
-
- Ding J, Li F, Huo L. Application of radionuclide imaging in patients with primary aldosteronism. Int J Radiat Med Nucl Med 2019;43:456-61.
LinkOut - more resources
Full Text Sources
Miscellaneous