

Triglyceride-glucose index threshold for cardiovascular mortality in hypertensive individuals - URRAH project
- PMID: 40687937
- PMCID: PMC12271081
- DOI: 10.1016/j.ajpc.2025.101053
Triglyceride-glucose index threshold for cardiovascular mortality in hypertensive individuals - URRAH project
Abstract
Aims: The triglyceride-glucose (TyG) index is a surrogate marker of insulin resistance (IR). Data regarding this topic is constantly increasing, however, few and heterogeneous data are available on the relationship between this index and cardiovascular mortality risk in hypertensive populations. In this context, we aimed to explore the relationship between TyG and cardiovascular mortality in a large sample of hypertensive individuals from the URRAH cohort.
Methods: A total of 12,275 hypertensive participants without previous cardiovascular events were included in this analysis. The risk of cardiovascular mortality was evaluated by the Cox regression analysis and competing risk regression analysis.
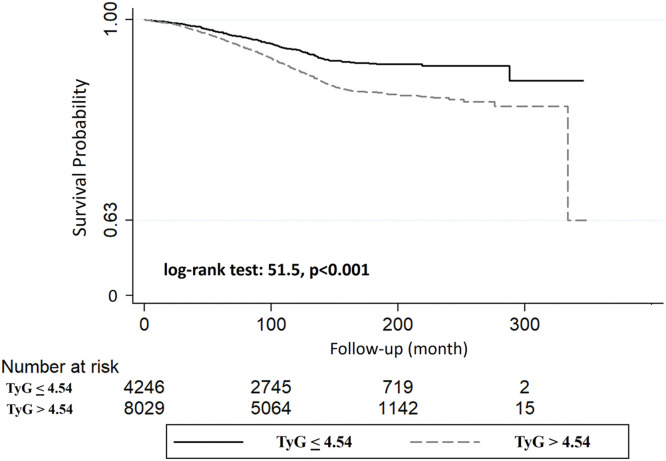
Results: During a median follow-up of 10.5 years, 2151 deaths occurred, of which 986 were from cardiovascular disease. A linear association between TyG and cardiovascular mortality was found, in particular for a 1-standard deviation increase in TyG there was a significantly increased risk of 33 % (p < 0.0001). Furthermore, after stratification by the optimal cut-off point (4.54 Units), participants with TyG above the cut-off had a significantly increased risk of 67 % of cardiovascular mortality when compared with those with TyG below the cut-off (p < 0.0001). These results were also confirmed after adjustment for potential confounders.
Conclusions: The results of this study indicate that this TyG threshold is predictive of an increased risk of cardiovascular mortality in a large sample of hypertensive individuals. This cut-off can identify individuals at higher mortality risk in already high-risk patients, with a low-cost and simple non-invasive marker.
Keywords: Cardiovascular mortality; Hypertension; Insulin resistance; Triglyceride-glucose index.
© 2025 The Authors. Published by Elsevier B.V.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: URRAH study group reports administrative support was provided by Fondazione of the Italian Society of Hypertension. Claudio Borghi reports a relationship with Menarini Corporate, Novartis Pharma, Alfasigma, Laboratoires Servier, Grunenthal, Takeda, Astellas, Teijin, Berlin Chemie, Sanofi that includes: consulting or advisory, funding grants, and speaking and lecture fees. The remaining authors have no disclosures to report.
Figures



References
-
- NCD Risk Factor Collaboration (NCD-RisC) Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021;398(10304):957–980. doi: 10.1016/S0140-6736(21)01330-1. Sep 11Epub 2021 Aug 24. Erratum in: Lancet. 2022 Feb 5;399(10324):520. 10.1016/S0140-6736(22)00061-7. - DOI - PMC - PubMed
-
- Kearney P.M., Whelton M., Reynolds K., Muntner P., Whelton P.K., He J. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365:217–223. - PubMed
-
- Sehestedt T., Hansen T.W., Li Y., Richart T., Boggia J., Kikuya M., Thijs L., Stolarz-Skrzypek K., Casiglia E., Tikhonoff V., Malyutina S., Nikitin Y., Björklund-Bodegård K., Kuznetsova T., Ohkubo T., Lind L., Torp-Pedersen C., Jeppesen J., Ibsen H., Imai Y., Wang J., Sandoya E., Kawecka-Jaszcz K., Staessen J.A. Are blood pressure and diabetes additive or synergistic risk factors? outcome in 8494 subjects randomly recruited from 10 populations. Hypertens Res. 2011;34(6):714–721. doi: 10.1038/hr.2011.6. Jun. - DOI - PubMed
-
- Lu S., Bao M.Y., Miao S.M., Zhang X., Jia Q.Q., Jing S.Q., Shan T., Wu X.H., Liu Y. Prevalence of hypertension, diabetes, and dyslipidemia, and their additive effects on myocardial infarction and stroke: a cross-sectional study in Nanjing, China. Ann Transl Med. 2019;7(18):436. doi: 10.21037/atm.2019.09.04. Sep. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
