

Optimizing primary tumor resection decisions for non-small cell lung cancer patients with brain metastases: analysis based on the SEER database and development and external validation of predictive models
- PMID: 40688268
- PMCID: PMC12268610
- DOI: 10.21037/jtd-24-1762
Optimizing primary tumor resection decisions for non-small cell lung cancer patients with brain metastases: analysis based on the SEER database and development and external validation of predictive models
Abstract
Background: Brain metastases (BM) in non-small cell lung cancer (NSCLC) are associated with poor prognosis, and the role of primary tumor resection (PTR) remains controversial. This study aims to evaluate the role of PTR in NSCLC patients with BM and develop a predictive tool to identify optimal surgical candidates.
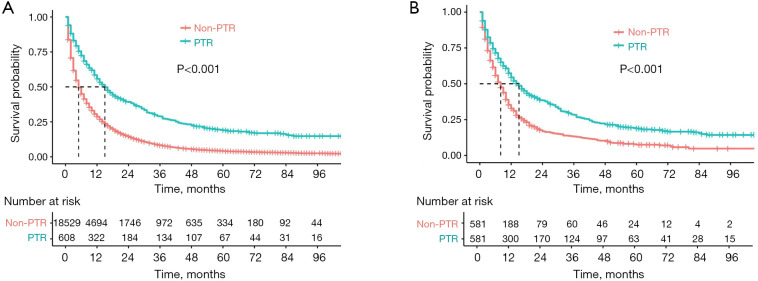
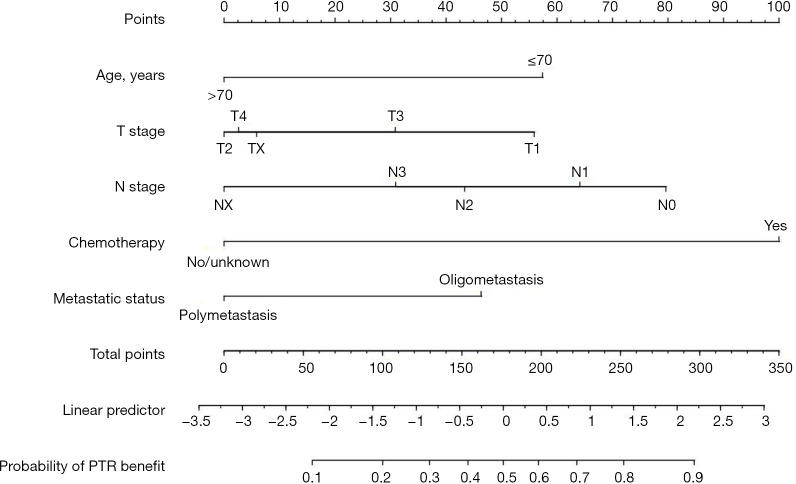
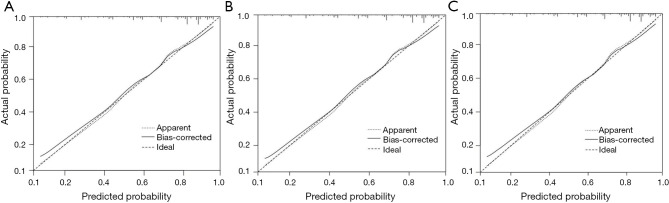
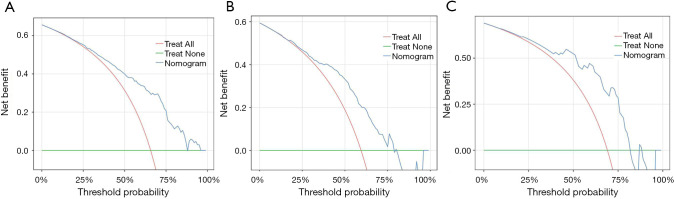
Methods: We analyzed data from 608 patients who underwent PTR and 18,529 patients who did not, sourced from the Surveillance, Epidemiology, and End Results (SEER) database. Propensity score matching (PSM), a statistical method to balance baseline characteristics between treatment groups, was performed to minimize selection bias. We utilized Kaplan-Meier (KM) survival analysis, Cox regression analysis, and PSM to assess the impact of PTR on the prognosis of BM patients. Logistic regression analysis was performed to identify and quantify the clinical factors that influence the benefits of PTR in BM patients, which informed the development of a predictive model. The model's predictive accuracy and clinical applicability were evaluated using the Concordance index (C-index), F1 score, receiver operating characteristic (ROC) curve, calibration curve, and decision curve analysis (DCA), with 42 patients from Fujian Provincial Hospital serving as the external validation cohort.
Results: KM survival analysis revealed significant survival differences between the PTR and non-PTR groups, both before and after PSM, with median survival times of 15 and 7 months, respectively. PTR was identified as an independent clinical factor affecting the prognosis of BM patients. In the training set, the C-index for the model was 0.7857 [95% confidence interval (CI): 0.7387-0.8327]. In the validation set, the C-index was 0.7441 (95% CI: 0.6674-0.8208), and in the external validation set, it was 0.7759 (95% CI: 0.5855-0.9662). The F1 score of the predictive model was 0.7667. Analyses of the ROC curve, calibration curve, and DCA indicated that the model exhibits strong accuracy and clinical applicability.
Conclusions: This study indicated that PTR can enhance the prognosis of NSCLC patients with BM and also establishes an effective screening tool for quantifying the likelihood of patient benefiting from PTR treatment.
Keywords: Non-small cell lung cancer (NSCLC); Surveillance, Epidemiology, and End Results (SEER); brain metastases (BM); primary tumor resection.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-24-1762/coif). The authors have no conflicts of interest to declare.
Figures




Similar articles
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
A novel nomogram for survival prediction in renal cell carcinoma patients with brain metastases: an analysis of the SEER database.Front Immunol. 2025 Jun 30;16:1572580. doi: 10.3389/fimmu.2025.1572580. eCollection 2025. Front Immunol. 2025. PMID: 40661946 Free PMC article.
-
Most eligible candidates for primary tumor resection among metastatic colorectal cancer patients: a SEER-based population analysis.Transl Cancer Res. 2025 Jul 30;14(7):4381-4398. doi: 10.21037/tcr-2025-1084. Epub 2025 Jul 24. Transl Cancer Res. 2025. PMID: 40792154 Free PMC article.
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.Health Technol Assess. 2006 Sep;10(34):iii-iv, ix-xi, 1-204. doi: 10.3310/hta10340. Health Technol Assess. 2006. PMID: 16959170
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous