

Unreliable sagittal T2-weighted flow void MRI in diagnosing third ventriculostomy: a case of long-standing obstructive hydrocephalus. Illustrative case
- PMID: 40690802
- PMCID: PMC12278952
- DOI: 10.3171/CASE2531
Unreliable sagittal T2-weighted flow void MRI in diagnosing third ventriculostomy: a case of long-standing obstructive hydrocephalus. Illustrative case
Abstract
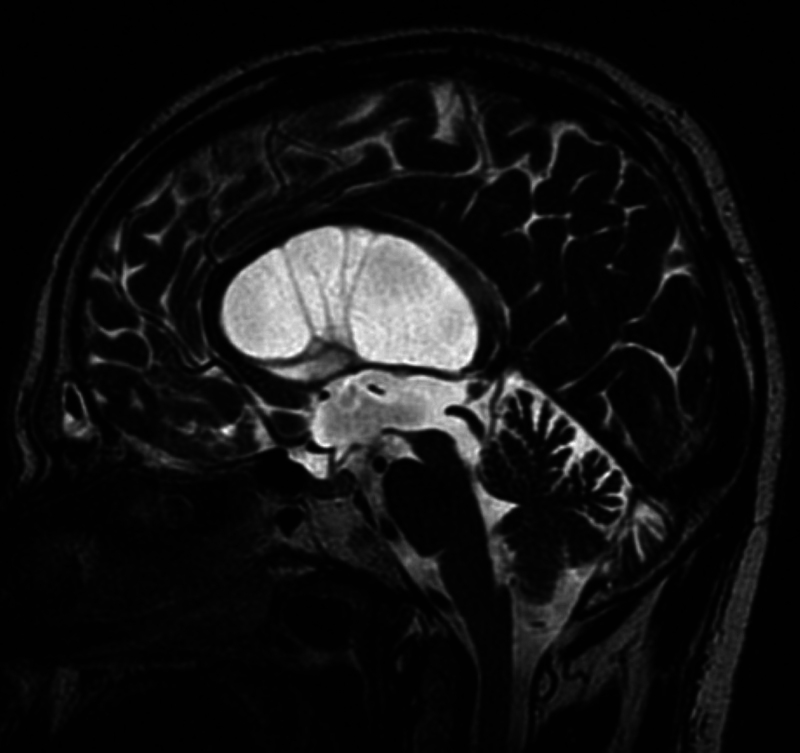
Background: Aqueductal stenosis represents one of the most common causes of CSF intraventricular blockage and may lead to obstructive triventricular hydrocephalus. In rare cases, the spontaneous rupture of the third ventricular floor, known as spontaneous third ventriculostomy (STV), can occur.
Observations: The authors report an illustrative case of pseudo-STV in a 67-year-old man who presented with long-standing obstructive triventricular hydrocephalus. Despite the neuroimaging findings suggesting STV, endoscopic third ventriculostomy showed an intact floor of the third ventricle.
Lessons: The authors demonstrate the potential for imaging to be misleading in the diagnosis of STV. A flow void artifact on sagittal T2-weighted sequences of the floor of the third ventricle may reflect the fast motion of a thin third ventricular floor or CSF passage through the foramen of Monro rather than flow void through a patent stoma. Endoscopic exploration remains the gold standard for confirming the presence of a ventriculostomy, but other noninvasive tools may help differentiate real CSF intraventricular motion. Dimensional phase-contrast velocity mapping like time-SLIP (arterial spin labeling) MRI could allow the differentiation of flow artifacts caused by the rapid motion of the pulsating floor of the third ventricle from a true ventriculostomy. https://thejns.org/doi/10.3171/CASE2531.
Keywords: aqueductal stenosis; endoscopic third ventriculostomy; hydrocephalus; neuroendoscopy; neurosurgery; spontaneous third ventriculostomy.
Figures




References
-
- Spennato P Tazi S Bekaert O Cinalli G Decq P.. Endoscopic third ventriculostomy for idiopathic aqueductal stenosis. World Neurosurg. 2013;79(2)(suppl):S21.e13-S21.e20. - PubMed
-
- Jellinger G.. Anatomopathology of non-tumoral aqueductal stenosis. J Neurosurg Sci. 1986;30(1-2):1-16. - PubMed
-
- Maller VV Gray RI.. Noncommunicating hydrocephalus. Semin Ultrasound CT MR. 2016;37(2):109-119. - PubMed
-
- Tisell M.. How should primary aqueductal stenosis in adults be treated? A review. Acta Neurol Scand. 2005;111(3):145-153. - PubMed
LinkOut - more resources
Full Text Sources
