

The effect of three different apical termini on postoperative pain in teeth with irreversible pulpitis: a prospective clinical study
- PMID: 40691618
- PMCID: PMC12278658
- DOI: 10.1186/s13005-025-00531-8
The effect of three different apical termini on postoperative pain in teeth with irreversible pulpitis: a prospective clinical study
Abstract
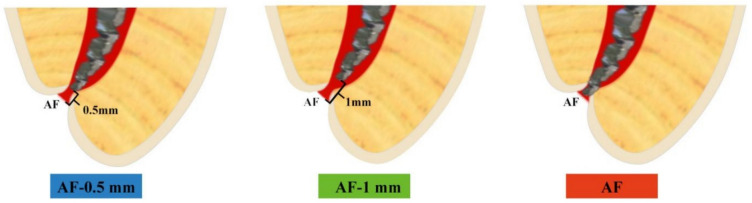
Background: The apical terminus of root canal preparation plays a critical role in minimizing postoperative pain. Yet, significant debate remains regarding the optimal termination point. This prospective clinical study aimed to assess the effect of three different apical termini on postoperative pain in teeth with irreversible pulpitis.
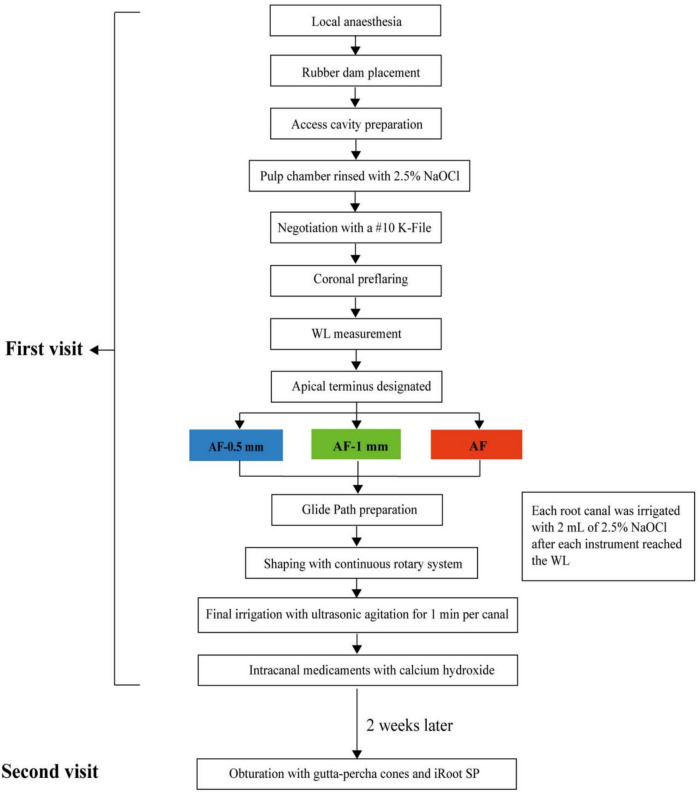
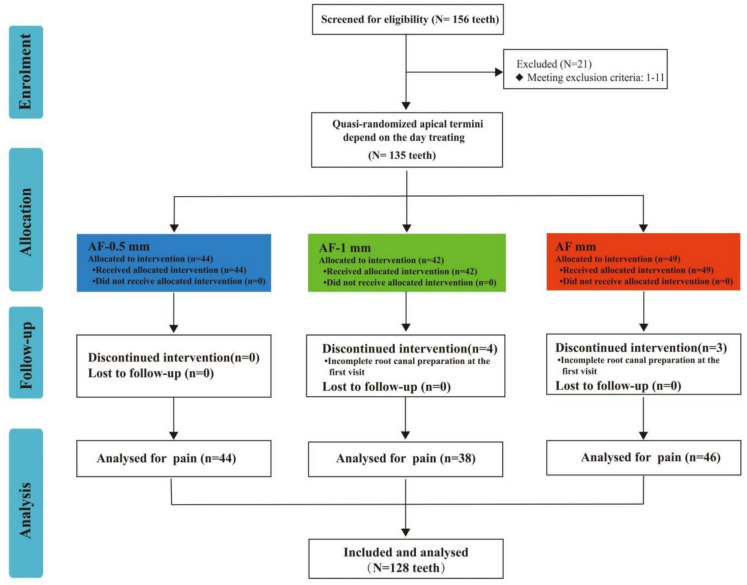
Methods: Totally, 128 patients with asymptomatic or symptomatic irreversible pulpitis were consecutively enrolled. Participants underwent root canal preparation with the apical terminus positioned either at the apical foramen (AF) or 0.5 or 1 mm short of it. Pain intensity was rated using an 11-point numerical rating scale (NRS-11) at nine time points. Data were analyzed using repeated measures analysis of variance.
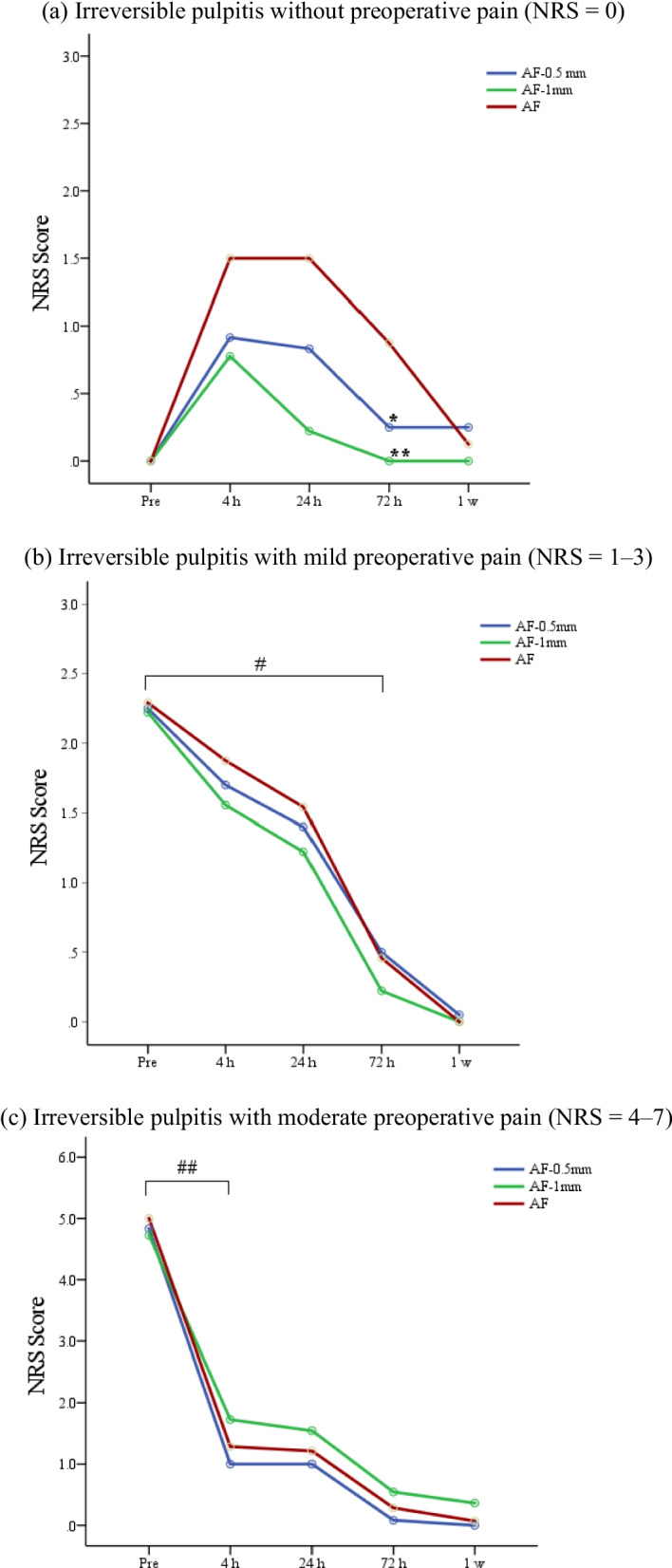
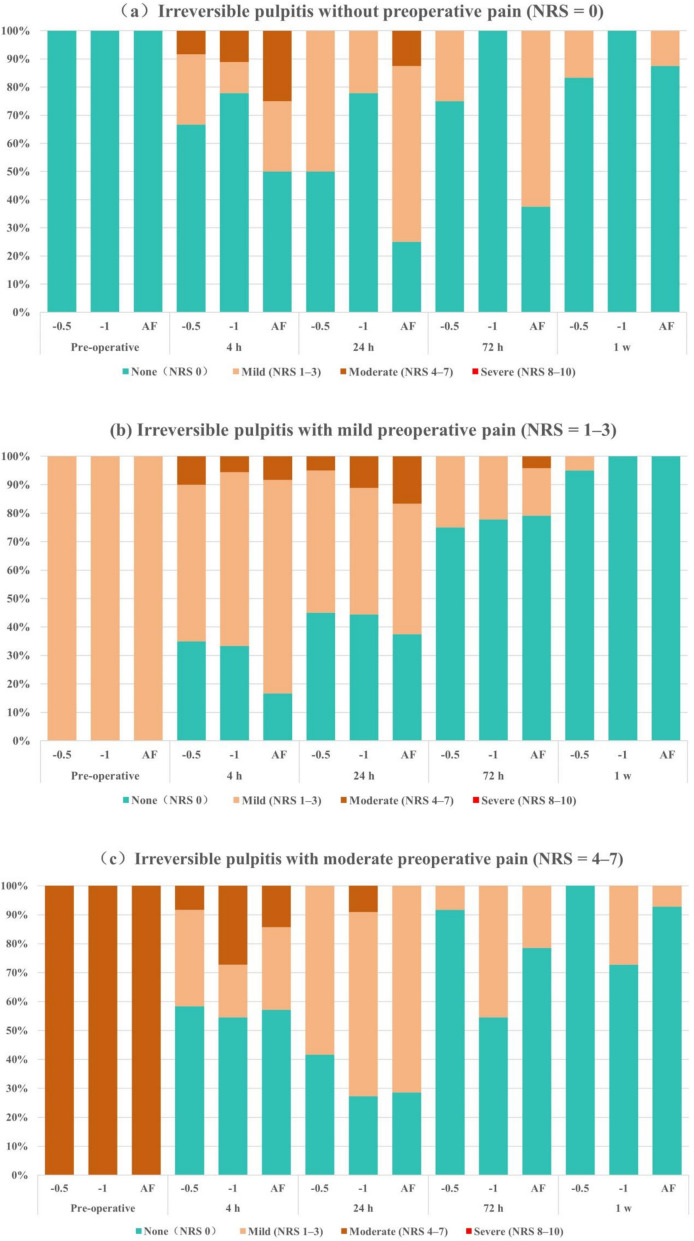
Results: In cases of irreversible pulpitis without preoperative pain (NRS = 0), the pain scores at 72 h after preparation were significantly lower in the AF-1 mm group than in the AF group (P < .05), with none of the patients in the AF-1 mm group reporting pain at this time point (P < .017). In cases of irreversible pulpitis with moderate preoperative pain (NRS = 4-7), the post-preparation pain scores at 4 h was significantly lower than the preoperative pain in all groups (P < .05). The pain scores in the AF-0.5 mm group remained lower than that in the other groups at 4 h, 24 h, 72 h, and 1 week. More patients reported decreased pain 4 h postoperatively in the AF-0.5 mm group than in other groups, with all patients in the AF-0.5 mm group reporting no pain at 1 week. In cases with mild preoperative pain (NRS = 1-3), the pain scores were significantly lower 72 h postoperatively than preoperatively (P < .05), with fewer patients reporting increased pain 24 h postoperatively in the AF-0.5 mm group than other groups.
Conclusions: Positioning the root canal apical terminus 0.5 and 1.0 mm short of the AF in symptomatic and asymptomatic cases of irreversible pulpitis, respectively, was most effective in reducing the severity and duration of postoperative pain. Tailoring apical preparation depth to the pulpal condition-symptomatic or asymptomatic-can optimize patient comfort and support more personalized endodontic care.
Keywords: Apical foramen; Apical terminus; Endodontic treatment outcomes; Irreversible pulpitis; Pain management; Postoperative pain; Root canal preparation.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The prospective clinical study was approved by the Institutional Review Board of Beijing Stomatological Hospital, Capital Medical University (No. CMUSH-IRB-KJ-PJ-2022–18) and registered at Medical Research (MR-11–22-005153). The study was conducted in accordance with the Declaration of Helsinki. All patients provided written informed consent to participate in the study. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- American Association of Endodontists. Glossary of endodontic terms. 10th ed. Chicago: American Association of Endodontists; 2020.
-
- Pak JG, White SN. Pain prevalence and severity before, during, and after root canal treatment: a systematic review. J Endod. 2011;37:429–38. 10.1016/j.joen.2010.12.016. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
